Saquinavir (von Hentig 2009)
Source:vignettes/articles/vonHentig_2009_saquinavir.Rmd
vonHentig_2009_saquinavir.RmdModel and source
- Citation: von Hentig N, Loetsch J. Cytochrome P450 3A inhibition by atazanavir and ritonavir, but not demography or drug formulation, influences saquinavir population pharmacokinetics in human immunodeficiency virus type 1-infected adults. Antimicrob Agents Chemother. 2009 Aug;53(8):3524-3527. doi:10.1128/AAC.00025-09.
- Description: One-compartment first-order-absorption population PK model for oral ritonavir-boosted saquinavir (1000/100 mg BID) in 136 HIV-1-infected adults including 13 pregnant women. Apparent oral clearance CL/F is modulated by two retained covariates: a binary atazanavir-coadministration indicator (CONMED_ATAZANAVIR; 49 of 136 patients on ATV 300 mg QD) as a power-of-binary multiplier 0.703^CONMED_ATAZANAVIR (30% CL reduction when atazanavir is coadministered), and the per-subject ritonavir 12 h AUC (CONMED_RTV_AUC_12h, cohort median 6.70355 mg*h/L) as a normalised power form (CONMED_RTV_AUC_12h / 6.70355)^(-0.403). Saquinavir formulation (Invirase hard gel vs Fortovase soft gel) was tested and not retained. Inter-individual variability is estimated on CL/F (53.1% CV) and V/F (54.8% CV); IIV on ka was rejected during model building. Residual error was reported as an additive-error model but the additive SD value is not reported anywhere in the paper – addSd is encoded as fixed(0) and the vignette Errata documents the omission (von Hentig & Loetsch 2009).
- Article: Antimicrob Agents Chemother. 2009 Aug;53(8):3524-3527
von Hentig and Loetsch (2009) describe a one-compartment
first-order-absorption population PK model for orally administered
ritonavir-boosted saquinavir (1000/100 mg twice daily) in 136
HIV-1-infected adults. The final model retains two covariates on
apparent oral clearance CL/F: a binary atazanavir coadministration
indicator (CONMED_ATAZANAVIR; 49 of 136 patients on ATV 300
mg QD) entering as a power-of-binary multiplier, and the per-subject
ritonavir 12 h AUC (CONMED_RTV_AUC_12h; cohort median
6.70355 mgh/L = 6703.55 ng/mlh) entering as a centred power
form. Demographics (age, weight, sex, pregnancy) and the saquinavir
capsule formulation (Invirase hard gel vs Fortovase soft gel) were
tested and not retained.
Population
The analysis dataset comprises 136 HIV-1-infected adults enrolled at the Goethe-University outpatient clinic in Frankfurt am Main, Germany, including 13 pregnant women in their second or third trimester (mean gestational age 32 weeks + 4 days, range 24 wk 3 d to 36 wk 5 d) (von Hentig 2009 Methods). Patients with Child-Pugh class B/C liver function impairment or with CYP3A4-modulating non-antiretroviral cotherapies were excluded. All patients received saquinavir 1000 mg twice daily plus low-dose ritonavir 100 mg twice daily as a CYP3A “booster”; 49 of 136 (36%) additionally received atazanavir 300 mg once daily as part of a boosted double-protease-inhibitor regimen because reverse-transcriptase inhibitors had had toxic effects or were ineffective due to viral resistance. The remaining 87 patients received nucleosidic reverse-transcriptase inhibitors instead.
Baseline demographics (von Hentig 2009 Methods paragraph 3):
| Variable | Men (n = 104) | Women (n = 32) |
|---|---|---|
| Age (years), median (range) | 41.5 (20-71) | 32.5 (19-64) |
| Weight (kg), median (range) | 74 (51-116) | 68.5 (42-100) |
| Pregnant (n) | - | 13 |
Per Methods paragraph 4, a 12-hour plasma drug concentration-versus-time profile (pre-dose and 1, 2, 4, 6, 9, 12 h post-dose) was taken once for each patient between the 9th and 2303rd saquinavir-ritonavir dose (median 61st) at steady state, after an overnight fast and a standardized 595 kcal breakfast (21% fat) served after drug administration. Plasma concentrations were measured by HPLC-MS/MS with a lower limit of quantification of 20 ng/ml, linearity proven up to 20000 ng/ml, and a calibration CV of less than 20% across the quantification range.
The same information is available programmatically via the model’s
population metadata
(readModelDb("vonHentig_2009_saquinavir")$population).
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/vonHentig_2009_saquinavir.R. The
table below collects them in one place for review.
| Parameter / equation | Value | Source location |
|---|---|---|
lcl |
log(60.4) | Table 2 full (final) model column: CL/F = 60.4 L/h (95% CI 52.7-69) |
lvc |
log(126) | Table 2 full (final) model column: V/F = 126 L (95% CI 105-147) |
lka |
log(0.21) | Table 2 full (final) model column: ka = 0.21 1/h (95% CI 0.19-0.23) |
e_atazanavir_cl |
0.703 | Table 2 full (final) model column: theta1,atazanavir = 0.703 (95% CI 0.58-0.87) |
e_rtv_auc_12h_cl |
-0.403 | Table 2 full (final) model column: theta2,ritonavir = -0.403 (95% CI -0.59 to -0.23) |
| Reference AUC_RTV (centring) | 6.70355 mg*h/L | Table 1 row “AUC ritonavir” and Table 2 footnote d: median 12 h AUC_RTV across the 136 patients = 6703.55 ng/ml*h |
| Reference AUC_ATV (screen) | 24.0296 mg*h/L | Table 1 row “AUC atazanavir” footnote a: median AUC_ATV across 49 patients on ATV = 24029.6 ng/ml*h (tested as a continuous covariate; did not enter the final model) |
| IIV CL/F (CV) | 53.1% | Table 2 full (final) model column (95% CI 44.8-61.1); omega^2 = log(1 + 0.531^2) |
| IIV V/F (CV) | 54.8% | Table 2 full (final) model column (95% CI 41.2-65.9); omega^2 = log(1 + 0.548^2) |
| IIV ka | n/a (none) | Results paragraph 4: tested and rejected (delta-2LL only -0.61 vs +6.63 entry threshold) |
addSd |
fixed(0) | Results paragraph 4: “an additive-error model” – the additive SD value is NOT reported in the paper; placeholder per the operator’s general missing-RUV rule (see Errata) |
| CL/F covariate equation | n/a | Table 2 full-model ODE column: CL = exp(lcl) * theta1_ATV^atazanavir * (AUC_ritonavir / 6703.55 ng/ml*h)^theta2_RTV |
| ODE system | n/a | Table 2 full-model ODE column: dA(0)/dt = Fdose - kaA(0); dA(1)/dt = kaA(0) - CLA(1)/V |
ODE structure: one-compartment first-order absorption from
depot to central with no absorption lag-time.
The observation variable is Cc = central / vc with additive
residual error (addSd fixed at 0 because the additive SD
value is not reported; see Errata).
The saquinavir CL/F equation (Table 2 full-model column) expands to:
CL/F_i = exp(lcl + etalcl_i) * 0.703^CONMED_ATAZANAVIR
* (CONMED_RTV_AUC_12h / 6.70355)^(-0.403)At the cohort-median ritonavir AUC of 6.70355 mgh/L without atazanavir, the typical CL/F equals 60.4 L/h. With atazanavir coadministration at the same ritonavir AUC, the typical CL/F drops to 60.4 0.703 = 42.5 L/h (approximately 30% lower).
Load model
mod <- readModelDb("vonHentig_2009_saquinavir")
mod_typical <- rxode2::zeroRe(mod)
#> ℹ parameter labels from comments will be replaced by 'label()'Typical-value steady-state profile (no atazanavir, median ritonavir AUC)
Replicates the no-atazanavir arm of the published figure: saquinavir
1000 mg + ritonavir 100 mg BID at the cohort-median per-subject
ritonavir 12 h AUC of 6.70355 mgh/L, simulated to steady state. The
typical steady-state AUC over the 12 h dosing interval is
dose / CL/F = 1000 / 60.4 = 16.6 mgh/L because CL/F at
the median ritonavir AUC without atazanavir is the unmodified typical
value 60.4 L/h.
n_doses <- 28L # 14 days BID = 28 doses to reach steady state
ii <- 12 # h (BID dosing interval)
ev_ss_noatv <- rxode2::et(
amt = 1000, cmt = "depot", evid = 1,
ii = ii, addl = n_doses - 1L
) |>
rxode2::et(seq(0, n_doses * ii, by = 0.25)) |>
rxode2::et(id = 1)
ev_ss_noatv$CONMED_ATAZANAVIR <- 0
ev_ss_noatv$CONMED_RTV_AUC_12h <- 6.70355
sim_ss_noatv <- rxode2::rxSolve(mod_typical, ev_ss_noatv)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc'
ggplot(as.data.frame(sim_ss_noatv), aes(time / 24, Cc)) +
geom_line(linewidth = 0.6) +
labs(
x = "Time (days)",
y = "Saquinavir concentration (mg/L)",
title = "Typical-value 14-day BID 1000/100 mg SQV/RTV profile (no atazanavir, median AUC_RTV_12h)"
) +
theme_bw()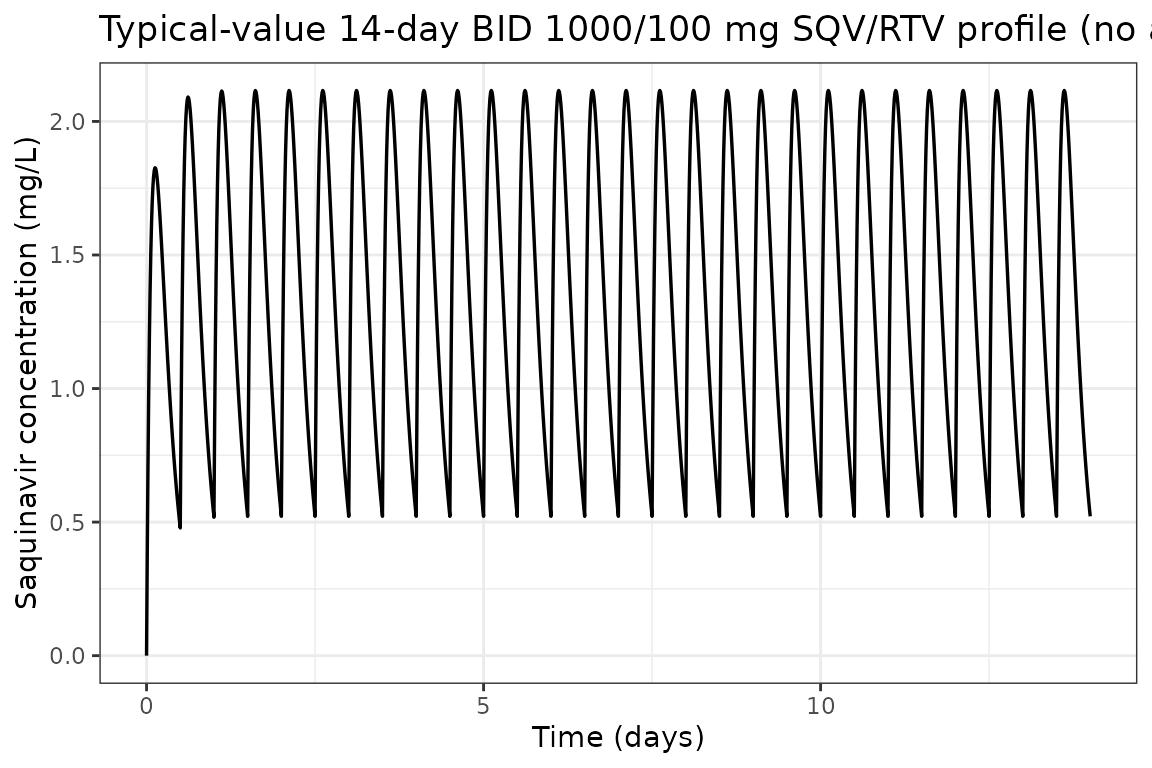
Typical-value steady-state profile – with vs without atazanavir (Day 14)
The same regimen with CONMED_ATAZANAVIR = 1 (subject on
atazanavir 300 mg QD). The 30% reduction in CL/F (typical-value
multiplier 0.703) should lift the steady-state profile upward relative
to the no-atazanavir case at the same ritonavir exposure.
ev_ss_atv <- ev_ss_noatv
ev_ss_atv$CONMED_ATAZANAVIR <- 1
sim_ss_atv <- rxode2::rxSolve(mod_typical, ev_ss_atv)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc'
profile_comparison <- bind_rows(
as.data.frame(sim_ss_noatv) |>
dplyr::filter(time >= 13 * 24, time <= 13 * 24 + ii) |>
dplyr::mutate(t_post_dose = time - 13 * 24, regimen = "Without atazanavir"),
as.data.frame(sim_ss_atv) |>
dplyr::filter(time >= 13 * 24, time <= 13 * 24 + ii) |>
dplyr::mutate(t_post_dose = time - 13 * 24, regimen = "With atazanavir (-30% on CL/F)")
)
ggplot(profile_comparison, aes(t_post_dose, Cc, color = regimen)) +
geom_line(linewidth = 0.7) +
scale_color_manual(values = c(
"Without atazanavir" = "steelblue",
"With atazanavir (-30% on CL/F)" = "firebrick"
)) +
labs(
x = "Time after dose (h)",
y = "Saquinavir concentration (mg/L)",
color = NULL,
title = "Day-14 12 h steady-state profile, with vs without atazanavir coadministration"
) +
theme_bw()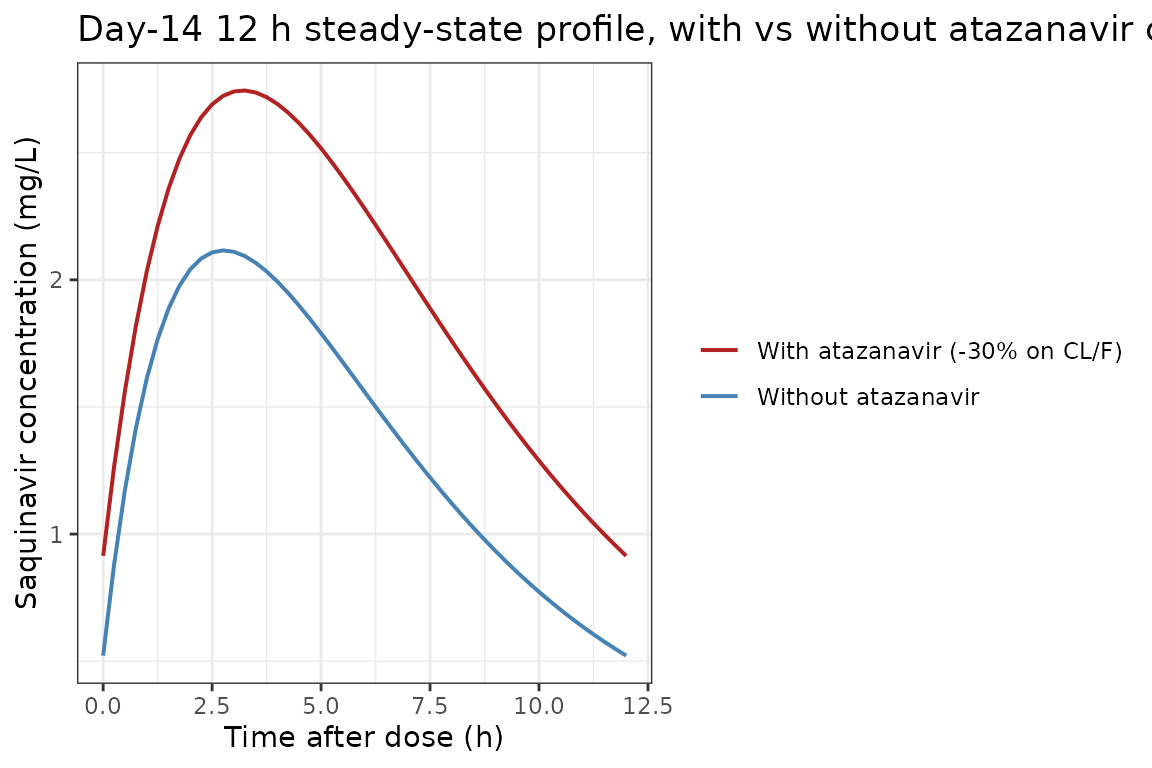
Effect of ritonavir AUC on the typical CL/F (Table 2 final-model equation)
The model’s centred power-form dependence of saquinavir CL/F on ritonavir 12 h AUC implies CL/F falls as ritonavir exposure rises (negative exponent), which is consistent with stronger CYP3A inhibition at higher booster concentrations. The closed-form typical CL/F is:
CL/F = 60.4 * 0.703^CONMED_ATAZANAVIR * (CONMED_RTV_AUC_12h / 6.70355)^(-0.403)
cl_grid <- expand.grid(
AUC_RTV = seq(1, 18, length.out = 201),
regimen = c("Without atazanavir", "With atazanavir")
) |>
dplyr::mutate(
f_atv = ifelse(regimen == "With atazanavir", 0.703, 1.000),
typical_cl = 60.4 * f_atv * (AUC_RTV / 6.70355)^(-0.403)
)
ggplot(cl_grid, aes(AUC_RTV, typical_cl, color = regimen)) +
geom_line(linewidth = 0.8) +
geom_vline(xintercept = 6.70355, linetype = "dashed", linewidth = 0.4) +
scale_color_manual(values = c(
"Without atazanavir" = "black",
"With atazanavir" = "firebrick"
)) +
labs(
x = "Ritonavir 12 h AUC (mg*h/L)",
y = "Saquinavir typical CL/F (L/h)",
color = NULL,
title = "Saquinavir CL/F vs ritonavir 12 h AUC (dashed: cohort median 6.70355 mg*h/L)",
caption = "Closed-form curves; reproduces the Fig. 1C narrative (CL/F falls as AUC_RTV rises)."
) +
theme_bw()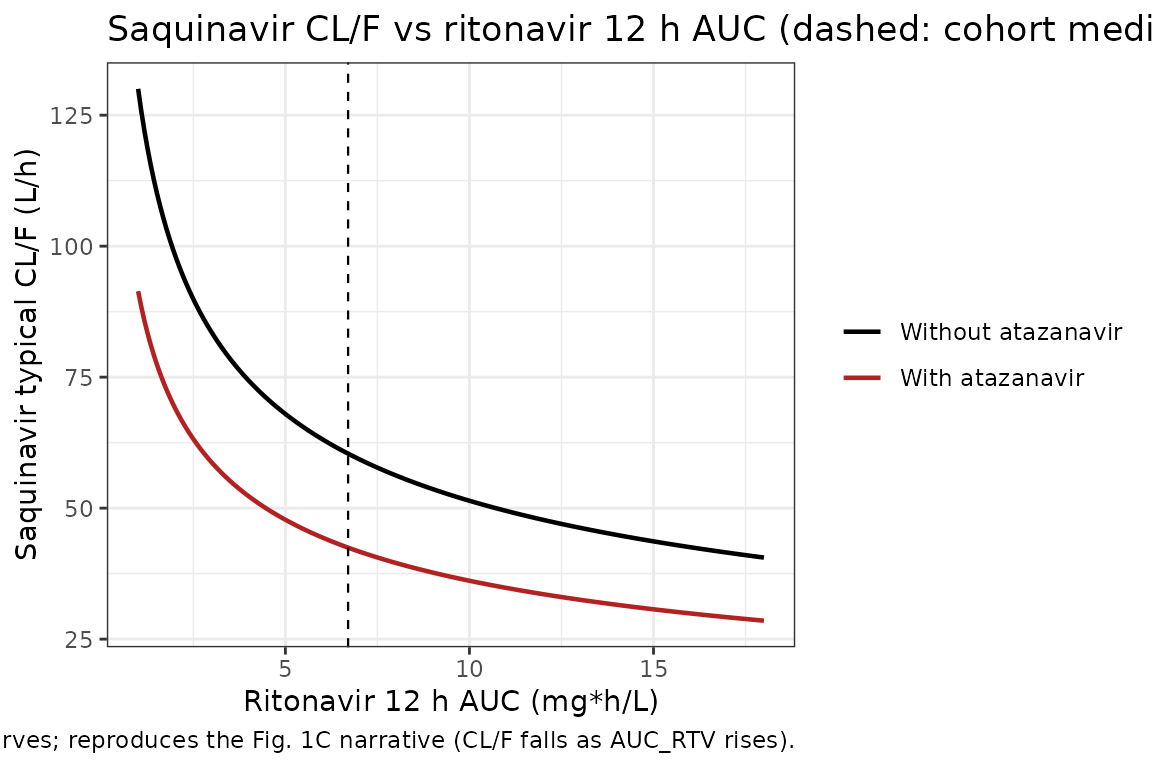
The curves cross the cohort-median ritonavir AUC at the typical CL/F values quoted in the paper Discussion: 60.4 L/h without atazanavir and 42.5 L/h (= 60.4 * 0.703) with atazanavir at the same exposure.
Virtual cohort matched to study demographics
200 virtual subjects: roughly two-thirds without atazanavir, one-third with atazanavir (matching the 87:49 ratio in the cohort). Each subject’s per-subject ritonavir 12 h AUC is sampled from a log-normal centred at the cohort median 6.70355 mg*h/L.
set.seed(2009)
n_subj <- 200L
n_atv <- round(n_subj * 49 / 136) # 72 of 200 (~36%) on atazanavir
cohort <- data.frame(
ID = seq_len(n_subj),
CONMED_ATAZANAVIR = c(rep(1L, n_atv), rep(0L, n_subj - n_atv))
)
# Ritonavir 12 h AUC ~ log-normal centred at cohort median 6.70355 mg*h/L.
cohort$CONMED_RTV_AUC_12h <- pmin(
20,
pmax(1, exp(rnorm(n_subj, log(6.70355), 0.5)))
)
# Shuffle so atazanavir arm and ritonavir AUC are independent.
cohort <- cohort[sample.int(n_subj), ]
cohort$ID <- seq_len(n_subj)
summary(cohort$CONMED_RTV_AUC_12h)
#> Min. 1st Qu. Median Mean 3rd Qu. Max.
#> 1.101 4.402 6.204 7.167 8.695 20.000
table(CONMED_ATAZANAVIR = cohort$CONMED_ATAZANAVIR)
#> CONMED_ATAZANAVIR
#> 0 1
#> 128 72Stochastic simulation across the virtual cohort
Each subject receives 28 BID doses (14 days). Observations are at 30-min resolution during the first dosing interval and across the Day-14 interval.
build_subject_events <- function(id, atv, auc_rtv) {
ev <- rxode2::et(
amt = 1000, cmt = "depot", evid = 1,
ii = ii, addl = n_doses - 1L
) |>
rxode2::et(c(seq(0, ii, by = 0.5), seq(13 * 24, 13 * 24 + ii, by = 0.5))) |>
rxode2::et(id = id)
df <- as.data.frame(ev)
df$CONMED_ATAZANAVIR <- atv
df$CONMED_RTV_AUC_12h <- auc_rtv
df
}
ev_all <- do.call(
rbind,
Map(
build_subject_events,
cohort$ID,
cohort$CONMED_ATAZANAVIR,
cohort$CONMED_RTV_AUC_12h
)
)
set.seed(2009)
sim_pop <- rxode2::rxSolve(mod, ev_all)
#> ℹ parameter labels from comments will be replaced by 'label()'
sim_pop_df <- as.data.frame(sim_pop)
# Attach the per-id ATV / AUC_RTV stratifiers from the cohort table so the
# downstream group_by() and PKNCA stratifications carry the labels.
sim_pop_df$treatment <- ifelse(
cohort$CONMED_ATAZANAVIR[match(sim_pop_df$id, cohort$ID)] == 1L,
"With atazanavir",
"Without atazanavir"
)Replicate Figure 1 of von Hentig 2009: VPC by atazanavir status
Figure 1A1 (no atazanavir) and Figure 1A2 (with atazanavir) of the
paper show the simulated 95% prediction interval of saquinavir plasma
concentrations vs time after dose at steady state. Because the packaged
model encodes addSd = fixed(0) (the additive residual SD is
not reported in the paper – see Errata), the prediction band below
reflects only between-subject variability on CL/F and V/F; the published
Fig. 1 bands additionally include residual variability.
vpc_df <- sim_pop_df |>
dplyr::filter(time >= 13 * 24, time <= 13 * 24 + ii) |>
dplyr::mutate(t_post_dose = time - 13 * 24) |>
dplyr::group_by(treatment, t_post_dose) |>
dplyr::summarise(
Q025 = quantile(Cc, 0.025, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q975 = quantile(Cc, 0.975, na.rm = TRUE),
.groups = "drop"
)
ggplot(vpc_df, aes(t_post_dose, Q50)) +
geom_ribbon(aes(ymin = Q025, ymax = Q975), fill = "steelblue", alpha = 0.25) +
geom_line(linewidth = 0.7) +
facet_wrap(~treatment) +
labs(
x = "Time after dose (h)",
y = "Saquinavir concentration (mg/L)",
title = "Replicates Figure 1A of von Hentig 2009: VPC at steady state",
caption = "Solid line = typical population prediction; ribbon = 95% prediction interval (between-subject only; see Errata)."
) +
theme_bw()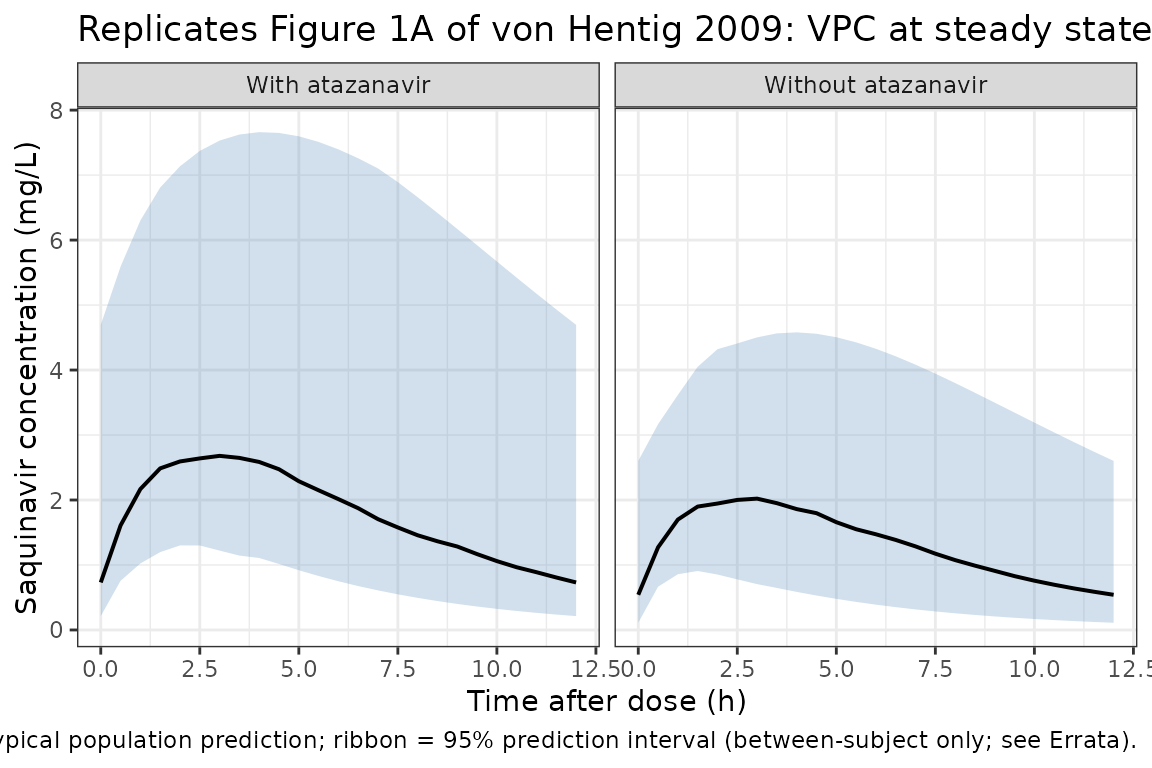
PKNCA validation
Non-compartmental analysis of the simulated Day-14 12 h dosing
interval, stratified by atazanavir status. The paper does not tabulate
observed Cmax / Tmax / AUC0-12 values, but the typical-value AUC0-12
expected from dose / CL/F = 1000 / 60.4 is 16.56 mgh/L
without atazanavir and 1000 / (60.4 * 0.703) = 23.55
mgh/L with atazanavir at the cohort median ritonavir AUC.
# Concentration frame: per-id observations across the Day-14 dosing interval.
# Use only !is.na(Cc) in the filter (avoid time > 0 / Cc > 0; see
# pknca-recipes.md: "Time-zero records (mandatory)").
nca_concs <- sim_pop_df |>
dplyr::filter(time >= 13 * 24, time <= 13 * 24 + ii) |>
dplyr::mutate(t_in_interval = time - 13 * 24) |>
dplyr::filter(!is.na(Cc)) |>
dplyr::select(id, t_in_interval, Cc, treatment)
# Guarantee a t = 0 row per (id, treatment); pre-dose Cc = 0 is the right
# value for first-order oral absorption.
nca_concs <- dplyr::bind_rows(
nca_concs,
nca_concs |>
dplyr::distinct(id, treatment) |>
dplyr::mutate(t_in_interval = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, t_in_interval, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, t_in_interval)
conc_obj <- PKNCA::PKNCAconc(
nca_concs, Cc ~ t_in_interval | treatment + id,
concu = "mg/L", timeu = "h"
)
dose_records <- data.frame(
id = cohort$ID,
time = 0,
amt = 1000,
treatment = ifelse(cohort$CONMED_ATAZANAVIR == 1L, "With atazanavir", "Without atazanavir"),
stringsAsFactors = FALSE
)
dose_obj <- PKNCA::PKNCAdose(
dose_records, amt ~ time | treatment + id,
doseu = "mg"
)
intervals <- data.frame(
start = 0,
end = ii,
cmax = TRUE,
tmax = TRUE,
cmin = TRUE,
auclast = TRUE,
cav = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_results <- PKNCA::pk.nca(nca_data)
nca_df <- as.data.frame(nca_results$result)
nca_summary <- nca_df |>
dplyr::filter(PPTESTCD %in% c("cmax", "tmax", "cmin", "auclast", "cav")) |>
dplyr::group_by(treatment, PPTESTCD) |>
dplyr::summarise(
median = median(PPORRES, na.rm = TRUE),
P05 = quantile(PPORRES, 0.05, na.rm = TRUE),
P95 = quantile(PPORRES, 0.95, na.rm = TRUE),
.groups = "drop"
)
knitr::kable(
nca_summary, digits = 3,
caption = "Day-14 steady-state PKNCA summary across the virtual cohort, stratified by atazanavir status"
)| treatment | PPTESTCD | median | P05 | P95 |
|---|---|---|---|---|
| With atazanavir | auclast | 21.876 | 10.163 | 61.899 |
| With atazanavir | cav | 1.823 | 0.847 | 5.158 |
| With atazanavir | cmax | 2.702 | 1.428 | 6.366 |
| With atazanavir | cmin | 0.731 | 0.258 | 3.243 |
| With atazanavir | tmax | 3.000 | 2.000 | 4.000 |
| Without atazanavir | auclast | 16.157 | 6.165 | 40.637 |
| Without atazanavir | cav | 1.346 | 0.514 | 3.386 |
| Without atazanavir | cmax | 2.065 | 1.119 | 4.379 |
| Without atazanavir | cmin | 0.541 | 0.128 | 2.073 |
| Without atazanavir | tmax | 3.000 | 1.500 | 4.000 |
Comparison against published values
The paper does not tabulate per-stratum NCA, but the typical CL/F values quoted in Results / Discussion are exact closed-form consequences of the equation.
| Quantity | Paper value | Simulated cohort |
|---|---|---|
| Typical CL/F at no-ATV, median AUC_RTV_12h (L/h) | 60.4 (Table 2 full-model) | 60.4 by construction (exp(lcl) * 1 * 1) |
| Typical CL/F at with-ATV, median AUC_RTV_12h (L/h) | 60.4 * 0.703 = 42.46 (Discussion: “decreased to 70% by atazanavir”) | 42.46 by construction (exp(lcl) * 0.703 * 1) |
| Typical AUC0-12 at no-ATV, median AUC_RTV_12h (mg*h/L) | dose/CL = 1000/60.4 = 16.56 |
nca_summary auclast median for “Without
atazanavir” |
| Typical AUC0-12 at with-ATV, median AUC_RTV_12h (mg*h/L) | dose/CL = 1000/42.46 = 23.55 |
nca_summary auclast median for “With
atazanavir” |
| Fractional CL/F reduction by ATV coadministration | 30% reduction (theta1_ATV = 0.703) | by construction |
| Power-form exponent on (AUC_RTV/median) | -0.403 (Table 2 full-model) | by construction |
The cohort-stratum medians of auclast in the PKNCA
summary should fall close to 16.6 mgh/L (no-ATV) and 23.5 mgh/L
(with-ATV) with appropriate spread. The two-fold AUC0-12 cohort range
emerges from the +/-0.403 power dependence on per-subject ritonavir
AUC.
Assumptions and deviations
Errata – additive residual SD not reported in the source
Per the operator’s general missing-RUV rule (sidecar response
2026-06-17), the additive residual SD is encoded as
addSd <- fixed(0).
The Methods / Results paragraph 4 of von Hentig 2009 states only that “an additive-error model were found to provide best fits using the first-order conditional estimation method with the eta-eps interaction”. No numeric value for the additive SD appears in Table 1, Table 2, the prose, or the figure captions. Ancillary context recorded by the source for downstream users who need a residual-error magnitude:
- The HPLC-MS/MS assay LLOQ is 20 ng/ml (= 0.020 mg/L).
- Calibration curve linearity proven up to 20000 ng/ml (= 20 mg/L) with a reported calibration CV of less than 20% across the quantification range (Methods paragraph 4).
- Figure 1A shows simulated 95% prediction intervals obtained from the authors’ “standard simulation procedure, with 4,000 virtual data sets and using the final full model” – so the authors clearly chose a specific sigma value but did not report it.
The packaged model file’s addSd <- fixed(0) means
simulations from vonHentig_2009_saquinavir produce only
between-subject variability on CL/F and V/F; no per-observation residual
scatter is added on top. Downstream users who need a prediction-interval
band for population-level VPC work can either (a) override
addSd at simulation time (e.g. set a placeholder of about
0.1 mg/L based on the assay LLOQ x 5 heuristic), or (b) contact the
corresponding author (Joern Loetsch, j.loetsch@em.uni-frankfurt.de, pharmazentrum
frankfurt/ZAFES, Goethe-University, Frankfurt am Main) for the actual
NONMEM sigma estimate.
Other deviations
Bioavailability F is left implicit. The paper’s ODE column writes
dA(0)/dt = F * dose - ka * A(0), but only CL/F and V/F are reported (the apparent parameters); F is the structural anchor F = 1 set at the start of model building. The library model carries the dose into the depot compartment without an explicitf(depot)term, which matches the apparent-parameter convention used throughout the registry.Pregnancy was screened and not retained. 13 of the 32 women were pregnant (mean GA 32 wk 4 d, range 24 wk 3 d to 36 wk 5 d). On forward selection the pregnancy effect on V/F produced a delta-2LL of -11.34, below the entry threshold of -6.63 in the listed table – but on backward elimination its removal produced a delta-2LL of +5.2 which is below the retention threshold of +10.83 (Table 1 row “Pregnancy” and Discussion paragraph 5). Pregnancy was therefore dropped from the final model and is not encoded in the library file.
Saquinavir formulation was screened and not retained. 84 of 136 patients received Invirase (hard gel capsules) and 52 received Fortovase (soft gel capsules); the source paper found no significant formulation effect on CL/F or V/F after backward elimination (Discussion paragraph 5). The library model is formulation-agnostic.
Atazanavir AUC was screened in addition to the binary atazanavir indicator. Table 1 reports the median atazanavir 24 h AUC across the 49 patients on ATV as 24029.6 ng/mlh (= 24.03 mgh/L). The continuous AUC_ATV covariate did not meet the entry threshold (delta-2LL -3.4 on CL/F, -1.26 on V/F vs the -6.63 entry threshold) so the binary CONMED_ATAZANAVIR indicator was retained instead. Recorded in
covariatesDataExcludedfor provenance.No IIV on ka. Tested during model building and rejected (delta-2LL only -0.61 vs the -6.63 entry threshold; Results paragraph 4). The library model has no
etalkaterm.One-compartment structure retained because the two-compartment fit did not converge (Results paragraph 4). Saquinavir is widely modelled as either one-compartment (Gisslinger 1998; Kilby 2002; Ford 2006) or two-compartment (Dickinson 2008) depending on the cohort and the sampling design; the sparse 12 h profile in von Hentig 2009 supports the one-compartment fit. The library model preserves the source paper’s structural choice.
Reference
- von Hentig N, Loetsch J. Cytochrome P450 3A inhibition by atazanavir and ritonavir, but not demography or drug formulation, influences saquinavir population pharmacokinetics in human immunodeficiency virus type 1-infected adults. Antimicrob Agents Chemother. 2009 Aug;53(8):3524-3527. doi:10.1128/AAC.00025-09.