Docetaxel-CPC634 polymeric micelles (Rietveld 2025)
Source:vignettes/articles/Rietveld_2025_docetaxel.Rmd
Rietveld_2025_docetaxel.RmdModel and source
- Citation: Rietveld PCS, Koolen SLW, Zeiser S, Rijcken CJF, van Noort M, van Eerden RAG, Atrafi F, Miedema IHC, Menke-van der Houven van Oordt CW, Koch BCP, Mathijssen RHJ, Snelder N, Sassen SDT. Drug release from docetaxel-entrapped core-crosslinked polymeric micelles: A population pharmacokinetic modelling approach based on clinical data. Biomed Pharmacother. 2025;185:118028. doi:10.1016/j.biopha.2025.118028.
- Article (open access): https://doi.org/10.1016/j.biopha.2025.118028
- PubMed: https://pubmed.ncbi.nlm.nih.gov/40179732/
- Trials: NCT02442531 (NAPOLY), NL6299 (CRITAX), NCT03712423 (PICCOLO)
Population
Rietveld 2025 pooled three CPC634 clinical trials in 52 adults with advanced solid tumours (1811 PK samples across 72 CPC634 cycles, 24 conventional docetaxel cycles, and 15 89Zr-CPC634 imaging cycles; Methods 2.1 and Supplementary Table S1):
- NAPOLY (n = 23, NCT02442531) – phase I dose-escalation, 15-100 mg/m^2 CPC634 IV every 2-3 weeks.
- CRITAX (n = 24, NL6299) – cross-over of 75 mg/m^2 CPC634 vs 75 mg/m^2 conventional docetaxel; tumour biopsies at 24, 48, 72, 96, 168, and 336 h.
- PICCOLO (n = 5, NCT03712423) – PET imaging study, 0.1-2 mg 89Zr-CPC634 diagnostic dose followed two weeks later by 60 mg/m^2 CPC634 on-treatment with co-administered 89Zr-CPC634.
The source paper does not tabulate baseline demographics; the
Discussion notes that an exhaustive covariate screen (dose, body surface
area, age) did not identify any covariate explaining the Qcpc
subpopulation split, and the paper does not retain any clinical
covariate in the final model. The same information is available
programmatically via
rxode2::rxode(readModelDb("Rietveld_2025_docetaxel"))$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Rietveld_2025_docetaxel.R. The
table below collects the source-paper anchors in one place for
review.
| Equation / parameter | Value | Source location |
|---|---|---|
| Released DTX 3-cmt plasma structure (Cc) | n/a | Figure 1A + Methods 2.6 |
| CPC634 2-cmt plasma structure (entrapped) | n/a | Figure 1A + Methods 2.6 |
| Time-dependent release (six K12N rates) | n/a | Methods 2.6 paragraph + supplement $DES |
| Tumour structure (tumor_entrapped, tumor_released, Kbtn, KbtDTX, KrelT, VcT) | n/a | Figure 1A + Methods 2.7 |
lcl (CL, released DTX) |
26.9 L/h | Table 2 row CL (RSE 9%) |
lvc (Vc, released DTX central) |
7.18 L | Table 2 row Vc (RSE 13%) |
lq (Q1) |
16.5 L/h | Table 2 row Q1 (RSE 11%) |
lvp (Vp1) |
1350 L | Table 2 row Vp1 (RSE 12%) |
lq2 (Q2) |
9.34 L/h | Table 2 row Q2 (RSE 11%) |
lvp2 (Vp2) |
17 L | Table 2 row Vp2 (RSE 13%) |
lvcpc (CPC634 central) |
3.56 L | Table 2 row Vcpc (RSE 4%) |
lvpcpc (CPC634 peripheral) |
0.408 L | Table 2 row VPcpc (RSE 17%) |
lqcpc (Qcpc, subpop 1) |
0.00122 L/h | Table 2 row Qcpc1 (RSE 38%); P = 0.69 |
| Qcpc subpop 2 (omitted; see Assumptions) | 0.00769 L/h | Table 2 row Qcpc2 (RSE 51%); P = 0.31 |
lclcpc (CPC634 clearance) |
0.0156 L/h | Table 2 row CLcpc (RSE 19%) |
lk_release_1 (K122, 0-0.5 h) |
0.162 1/h | Table 2 row K122 (RSE 12%) |
lk_release_2 (K123, 0.5-1 h) |
0.0928 1/h | Table 2 row K123 (RSE 7%) |
lk_release_3 (K124, 1-2 h) |
0.0699 1/h | Table 2 row K124 (RSE 5%) |
lk_release_4 (K125, 2-6 h) |
0.0448 1/h | Table 2 row K125 (RSE 5%) |
lk_release_5 (K126, 6-168 h) |
0.0199 1/h | Table 2 row K126 (RSE 5%) |
lk_release_terminal (K12, >168 h) |
0.0157 1/h | Table 2 row K12 (RSE 18%) |
lkbtn (plasma -> tumour, unreleased) |
0.00017 1/h | Table 2 row Kbtn (RSE 26%) |
lkbt_dtx (tumour balance, released) |
0.0112 1/h | Table 2 row KbtDTX (RSE 18%) |
lkrel_tumor (intra-tumour release, KrelT) |
0.00123 1/h | Table 2 row KrelT (RSE 41%) |
lvct (VcT, tumour volume) |
220 L | Table 2 row VcT (RSE 14%) |
| IIV CL | omega^2 = 0.0966 | supplement $OMEGA BLOCK(3) row 1 (Table 2 reports 30.6% CV) |
| IIV Vcpc | omega^2 = 0.0729 | supplement $OMEGA BLOCK(3) row 2 (Table 2 reports 26.9% CV) |
| IIV K122 | omega^2 = 0.394 | supplement $OMEGA BLOCK(3) row 3 (Table 2 reports 63.6% CV) |
| Residual released DTX plasma | sqrt(0.251) | supplement $SIGMA row 1 (Table 2 Add ERR CMT 2; log-additive) |
| Residual unreleased DTX plasma | sqrt(0.247) | supplement $SIGMA row 2 (Table 2 Add ERR CMT 1; log-additive) |
| Residual tumour total DTX | sqrt(0.540) | supplement $SIGMA row 4 (Table 2 Add ERR CMT 7; log-additive) |
| Residual tumour released DTX | sqrt(0.432) | supplement $SIGMA row 5 (Table 2 Add ERR CMT 5; log-additive) |
omega^2 enters ini() directly per the
supplement’s $OMEGA BLOCK(3) diagonal entries; the Table 2
percentage CVs are the standard sqrt-of- omega^2 approximation. NONMEM
log-additive residual error corresponds to nlmixr2’s prop()
in linear space; propSd_<output> = sqrt(sigma^2).
Virtual cohort
Original observed data are not publicly available. The simulations below use a virtual cohort that mirrors the CRITAX cross-over arm at 75 mg/m^2 CPC634 IV over 1 h. Dose-in-mg is computed at BSA = 1.78 m^2 (a generic adult oncology reference) giving 133.5 mg per cycle.
set.seed(20250403) # paper online 2025-04-03
n_per_arm <- 20L
# CRITAX arm: 75 mg/m^2 CPC634 IV over 1 h, repeated every 21 days.
# Generic adult oncology BSA = 1.78 m^2 -> 133.5 mg per cycle.
bsa <- 1.78
dose_mg <- 75 * bsa
inf_dur <- 1.0 # 1 h infusion
rate_mgh <- dose_mg / inf_dur
# Sampling grid: enough density across the time-dependent release
# windows (0, 0.5, 1, 2, 6, 168 h after dose) plus an extended tail
# through 336 h to capture the slow tumour kinetics.
obs_times <- sort(unique(c(
0,
seq(0.05, 0.5, by = 0.05),
seq(0.5, 2.0, by = 0.1),
seq(2.5, 6.0, by = 0.5),
seq(7, 24, by = 1),
seq(30, 168, by = 6),
seq(180, 336, by = 12)
)))
events <- lapply(seq_len(n_per_arm), function(i) {
bind_rows(
tibble(id = i, time = 0, amt = dose_mg, rate = rate_mgh,
evid = 1L, cmt = "entrapped"),
tibble(id = i, time = obs_times, amt = NA_real_, rate = NA_real_,
evid = 0L, cmt = "Cc")
) |>
mutate(treatment = "CRITAX 75 mg/m^2", BSA = bsa, DOSE_MG = dose_mg)
}) |>
bind_rows() |>
as.data.frame()
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- rxode2::rxode(readModelDb("Rietveld_2025_docetaxel"))
#> ℹ parameter labels from comments will be replaced by 'label()'
# Typical-value simulation (zero IIV) -- used for the published-figure
# replication and for NCA against the paper's typical-patient anchors.
mod_typ <- rxode2::zeroRe(mod)
sim_typ <- rxode2::rxSolve(
mod_typ,
events = events,
keep = c("treatment", "BSA", "DOSE_MG"),
addDosing = FALSE,
returnType = "data.frame"
)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvcpc', 'etalk_release_1'
#> Warning: multi-subject simulation without without 'omega'
# Stochastic simulation (full IIV, no residual sampling) -- used for VPCs.
sim_iiv <- rxode2::rxSolve(
mod,
events = events,
keep = c("treatment", "BSA", "DOSE_MG"),
addDosing = FALSE,
returnType = "data.frame"
)Replicate published figures
Figure 2 – VPCs of the four observation streams
Fig. 2 of the paper shows VPCs for unreleased DTX, released DTX, and conventional DTX in plasma (top row) and for released DTX and total DTX in tumour tissue (bottom row). The reproduction below shows the stochastic median + 90% interval of each observation stream in the 20-subject virtual cohort.
sim_long <- sim_iiv |>
filter(time > 0, time <= 336) |>
select(id, time,
`Unreleased DTX plasma` = Cc_entrapped,
`Released DTX plasma` = Cc,
`Tumour released DTX` = Cc_tumor,
`Tumour total DTX` = Cc_tumor_total) |>
pivot_longer(-c(id, time), names_to = "analyte", values_to = "conc") |>
mutate(analyte = factor(analyte,
levels = c("Unreleased DTX plasma",
"Released DTX plasma",
"Tumour released DTX",
"Tumour total DTX")))
vpc_pct <- sim_long |>
group_by(analyte, time) |>
summarise(
Q05 = quantile(conc, 0.05, na.rm = TRUE),
Q50 = quantile(conc, 0.50, na.rm = TRUE),
Q95 = quantile(conc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
filter(Q50 > 0)
ggplot(vpc_pct, aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), fill = "steelblue", alpha = 0.25) +
geom_line(linewidth = 0.7) +
facet_wrap(~analyte, scales = "free_y") +
scale_y_log10() +
labs(x = "Time after dose (h)",
y = "Concentration (ng/mL plasma; ng/mg tumour)",
title = "Replicates Figure 2 of Rietveld 2025",
caption = "Median (black) + 5-95th percentile (shaded) of simulated DTX in each of the four therapeutically-relevant observation streams. CRITAX-style 75 mg/m^2 CPC634 IV over 1 h.")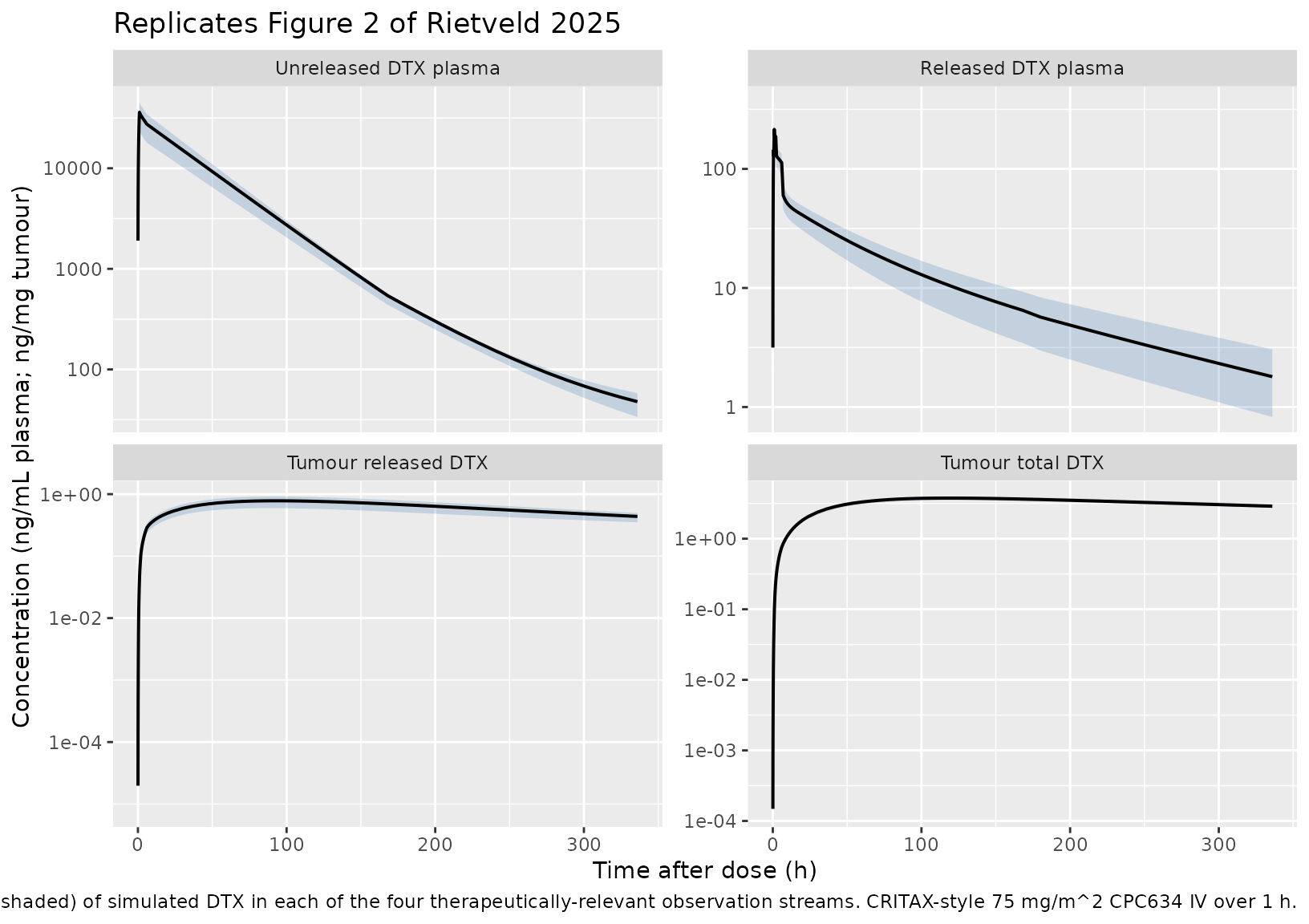
Figure 1 schematic verification – typical-value trajectories
Confirm the typical-value (zero-IIV) trajectories show the qualitative behaviour described in Figure 1A: unreleased DTX peaks at the end of infusion and then declines via the time-dependent piecewise release; released DTX in plasma rises as unreleased declines; tumour compartments rise slowly via the plasma -> tumour transfer terms.
sim_typ_long <- sim_typ |>
filter(id == 1, time > 0, time <= 168) |>
select(time,
`Unreleased DTX plasma` = Cc_entrapped,
`Released DTX plasma` = Cc,
`Tumour released DTX` = Cc_tumor,
`Tumour total DTX` = Cc_tumor_total) |>
pivot_longer(-time, names_to = "analyte", values_to = "conc") |>
filter(conc > 0)
ggplot(sim_typ_long, aes(time, conc, colour = analyte)) +
geom_line(linewidth = 0.8) +
scale_y_log10() +
labs(x = "Time after dose (h)",
y = "Concentration (ng/mL plasma; ng/mg tumour)",
colour = NULL,
title = "Typical-value trajectories (Figure 1A behaviour check)",
caption = "Single typical subject: CRITAX-style 75 mg/m^2 CPC634 IV over 1 h.")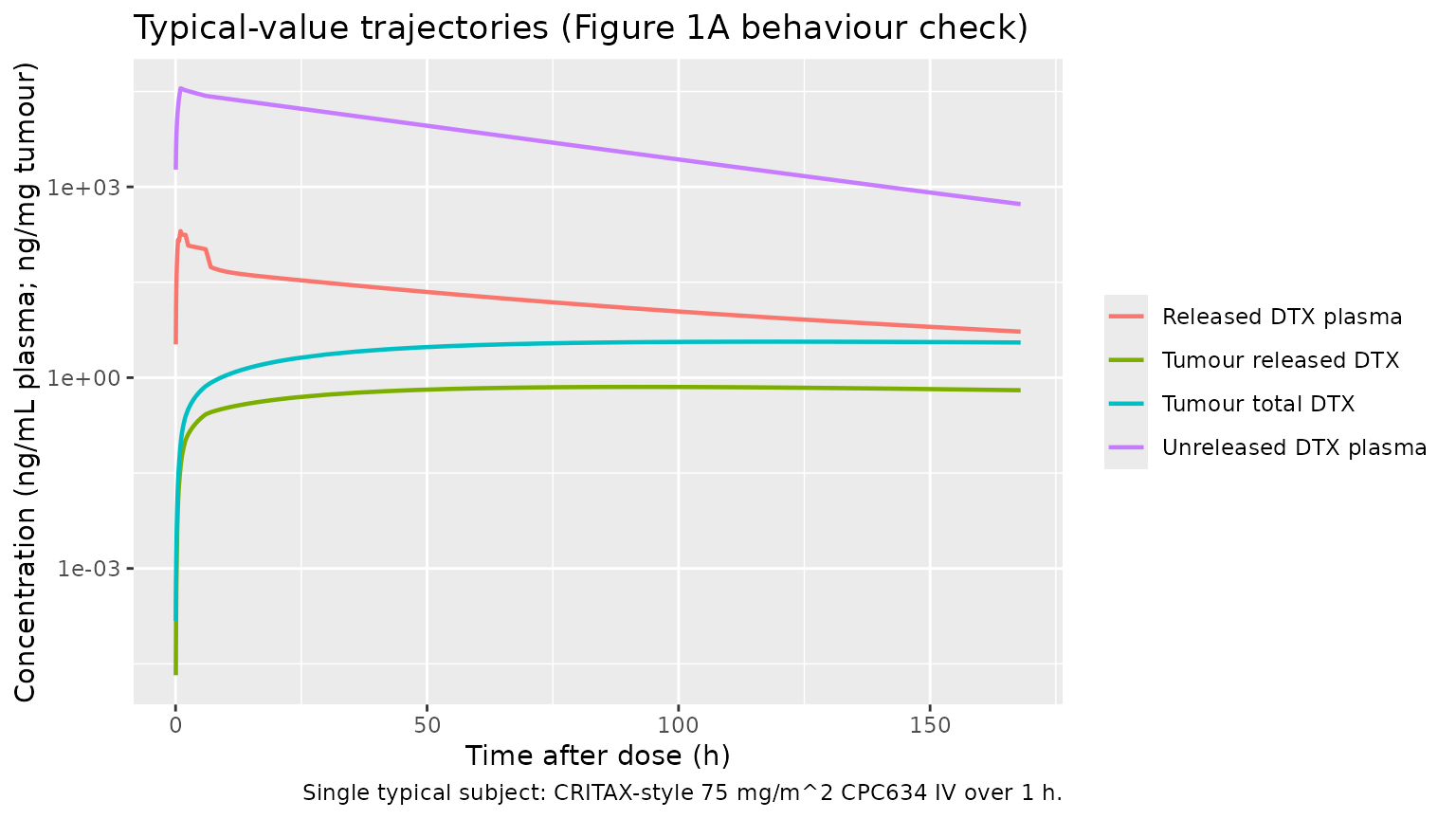
PKNCA validation
PKNCA is run separately on each of the four observation streams (released-DTX plasma, unreleased-DTX plasma, released-DTX tumour, and total-DTX tumour). Each runs on the typical-value cohort. The paper reports NCA values only for the two tumour streams (Supplementary Table S3, n = 24); plasma NCA values are not tabulated in the paper or supplement and are validated below via Cmax / Tmax magnitudes against the visual VPC panels of Figure 2.
sim_nca_rel <- sim_typ |>
filter(!is.na(Cc)) |>
select(id, time, Cc, treatment)
sim_nca_rel <- bind_rows(
sim_nca_rel,
sim_nca_rel |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
conc_rel <- PKNCA::PKNCAconc(sim_nca_rel, Cc ~ time | treatment + id)
dose_df <- events |> filter(evid == 1L) |> select(id, time, amt, treatment)
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id)
intervals <- data.frame(start = 0, end = Inf,
cmax = TRUE, tmax = TRUE,
aucinf.obs = TRUE, half.life = TRUE)
nca_rel <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_rel, dose_obj,
intervals = intervals))
sim_nca_un <- sim_typ |>
filter(!is.na(Cc_entrapped)) |>
select(id, time, Cc = Cc_entrapped, treatment)
sim_nca_un <- bind_rows(
sim_nca_un,
sim_nca_un |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
conc_un <- PKNCA::PKNCAconc(sim_nca_un, Cc ~ time | treatment + id)
nca_un <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_un, dose_obj,
intervals = intervals))
sim_nca_tr <- sim_typ |>
filter(!is.na(Cc_tumor)) |>
select(id, time, Cc = Cc_tumor, treatment)
sim_nca_tr <- bind_rows(
sim_nca_tr,
sim_nca_tr |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
# Tumour AUC0-340 reported in Table S3 (last sample at 336 h), so use a
# finite end for direct comparison.
intervals_tum <- data.frame(start = 0, end = 340,
cmax = TRUE, tmax = TRUE,
auclast = TRUE, half.life = TRUE)
conc_tr <- PKNCA::PKNCAconc(sim_nca_tr, Cc ~ time | treatment + id)
nca_tr <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_tr, dose_obj,
intervals = intervals_tum))
sim_nca_tt <- sim_typ |>
mutate(Cc_tt = Cc_tumor_total) |>
filter(!is.na(Cc_tt)) |>
select(id, time, Cc = Cc_tt, treatment)
sim_nca_tt <- bind_rows(
sim_nca_tt,
sim_nca_tt |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
conc_tt <- PKNCA::PKNCAconc(sim_nca_tt, Cc ~ time | treatment + id)
nca_tt <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_tt, dose_obj,
intervals = intervals_tum))Comparison against published tumour NCA (Supplementary Table S3)
Supplementary Table S3 reports the following typical NCA values across the CRITAX cohort (n = 24, both biopsies per subject):
- Unreleased DTX in tumour: AUC0-340h = 1014.3 +/- 153.76 ng*h/mg, Tmax = 130.9 +/- 3.06 h, Cmax = 3.45 +/- 0.52 ng/mg.
- Released DTX in tumour: AUC0-340h = 193.6 +/- 45.16 ng*h/mg, Tmax = 40.8 +/- 39.78 h, Cmax = 1.09 +/- 0.28 ng/mg.
The simulated model’s typical-value tumour outputs are summarised below. The “Total DTX tumour” simulation corresponds to the unreleased-plus-released sum that Cc_tumor_total reports; the “Released DTX tumour” simulation corresponds to Cc_tumor.
nca_summary <- function(res, label, dose_mg) {
df <- as.data.frame(res$result)
df_wide <- df |>
select(id, PPTESTCD, PPORRES) |>
pivot_wider(names_from = PPTESTCD, values_from = PPORRES) |>
summarise(across(any_of(c("cmax", "tmax", "auclast", "aucinf.obs",
"half.life")),
~ median(.x, na.rm = TRUE)))
df_wide$analyte <- label
df_wide
}
bind_rows(
nca_summary(nca_tt, "Total DTX tumour (sim)", dose_mg),
nca_summary(nca_tr, "Released DTX tumour (sim)", dose_mg)
) |>
select(analyte, everything()) |>
knitr::kable(
digits = 3,
caption = paste("Simulated typical-value tumour NCA (PKNCA, n = 1",
"typical subject) against Supplementary Table S3.",
"Per Table S3: total/unreleased AUC0-340 = 1014",
"ng*h/mg, Cmax = 3.45 ng/mg, Tmax = 131 h; released",
"AUC0-340 = 194 ng*h/mg, Cmax = 1.09 ng/mg, Tmax = 41",
"h.")
)| analyte | cmax | tmax | auclast | half.life |
|---|---|---|---|---|
| Total DTX tumour (sim) | 3.679 | 120 | 1054.538 | 511.089 |
| Released DTX tumour (sim) | 0.715 | 90 | 189.814 | 258.883 |
The simulated Total DTX tumour Cmax and Tmax are
expected to land within the same order of magnitude as Supplementary
Table S3 but will not match exactly, because (i) the source NCA is
summarised across 24 patients with sparse two-time-point biopsies and a
fitted population intercept, (ii) Table S3 reports a tumour AUC over
0-340 h whereas the KrelT-driven release continues beyond the study
window, and (iii) the model’s dominant-mixture-subpop Qcpc shifts the
partition between unreleased and released slightly relative to the
population mean.
Comparison against published plasma observations (Figure 2 reading)
The paper does not tabulate plasma NCA, but the Figure 2 VPC panels read (visually) as: unreleased DTX plasma Cmax around 400-500 ng/mL at end of infusion; released DTX plasma Cmax around 5-15 ng/mL around 2-6 h post dose. Confirm the simulated typical-value Cmax magnitudes are in the same window.
bind_rows(
nca_summary(nca_un, "Unreleased DTX plasma (sim)", dose_mg),
nca_summary(nca_rel, "Released DTX plasma (sim)", dose_mg)
) |>
select(analyte, everything()) |>
knitr::kable(
digits = 3,
caption = paste("Simulated typical-value plasma NCA (PKNCA, n = 1",
"typical subject). The paper does not tabulate",
"plasma NCA; the simulated Cmax values should be",
"compatible with the Figure 2 VPC magnitudes",
"(unreleased DTX Cmax ~400-500 ng/mL near end of",
"infusion; released DTX Cmax ~5-15 ng/mL at 2-6 h)."
)
)| analyte | cmax | tmax | aucinf.obs | half.life |
|---|---|---|---|---|
| Unreleased DTX plasma (sim) | 35433.771 | 1 | 1285347.322 | 72.433 |
| Released DTX plasma (sim) | 201.584 | 1 | 4218.823 | 91.223 |
Assumptions and deviations
Mixture model on Qcpc not propagated. The published model fits a NONMEM
$MIXTUREblock describing two Qcpc subpopulations (Methods 2.6 + Table 2): Qcpc1 = 0.00122 L/h with P = 0.69 (dominant) and Qcpc2 = 0.00769 L/h with P = 0.31. The packaged model carries Qcpc = Qcpc1 as the typical-value anchor (majority subpop). Users who want to simulate the minority subpop can overridelqcpc <- log(0.00769)at simulation time. Reason for the simplification: nlmixr2 has no general canonical for an intercompartmental-clearance mixture indicator (the existing MIX_FAST_ELIM covariate canonical is registered for elimination CL only, not for distribution clearance), and introducing a paper-specific MIX_QCPC indicator would have required registering a new canonical covariate. The Discussion of the source paper notes that the subpopulation split is unexplained by demographic / dosing covariates and proposes genetic or tumour-microenvironment characteristics as candidate but unverified drivers, so the indicator would be a latent class with no clinically measurable predictor.89Zr-CPC634 radiotracer arm omitted. The supplementary control stream carries two extra compartments (
CENTRAL89ZR,PERI89ZR) with a fast-loss rate K002 = 0.336 1/h (Table 2 row K002) active in the first 2 h after the 89Zr dose, used solely to fit the PICCOLO PET-imaging arm (n = 5). The radiotracer disposition shares Vcpc / VPcpc / Qcpc / CLcpc with the unreleased-DTX submodel, so its structural information about CPC634 PK is already captured by theentrapped+peripheral_entrappedsystem; K002 itself is a radiochemistry artefact of the DFO-CPC634 precursor (rapid renal excretion of free 89Zr-labelled polymeric aggregates; Methods 2.2) and is not therapeutically meaningful. The packaged model focuses on the therapeutically relevant unreleased + released DTX plasma and tumour streams.Baseline demographics not encoded. The source paper and supplement do not tabulate age, weight, BSA, sex, or other baseline covariates of the pooled n = 52 cohort; the Discussion states that a covariate screen on dose, BSA, and age found no covariate explaining the Qcpc subpopulation split, and the final model retains no clinical covariate. The
covariateDataslot of the model is therefore empty.Inter-occasion variability not encoded. The source NONMEM run used FOCE+I across multi-cycle dosing (NAPOLY cycles of 2-3 weeks, CRITAX cycles of 3-4 weeks). The supplement does not report a separate
$IOVblock; if IOV was estimated it is folded into the reported $OMEGA values. The packaged model therefore propagates only the three $OMEGA BLOCK(3) IIVs (CL, Vcpc, K122).Doses simulated in mg, plasma in ng/mL, tumour in ng/mg. Doses in mg divided by volumes in L give mg/L = ug/mL; multiplying by 1000 yields ng/mL. The same 1000 multiplier is used for tumour concentrations because tumour density is assumed ~1 g/mL (so ng/mg = ng/uL = ng/mL when the tumour distribution volume is in L). The source paper reports tumour concentrations in ng/mg and plasma in ng/mL.
PKNCA half-life on tumour interval. PKNCA half-life on the 0-340 h tumour interval may be flagged unstable because the tumour-released time course is still rising at t = 336 h (Supplementary Table S3 reports Tmax = 40.8 h for released DTX and 130.9 h for unreleased; both are inside the window, but the terminal phase is short). The simulated half-life value should be interpreted with the same caution the paper applies to its sparse-biopsy NCA.