Sugammadex-mediated reversal of rocuronium NMB (Kleijn 2011)
Source:vignettes/articles/Kleijn_2011_sugammadex_rocuronium.Rmd
Kleijn_2011_sugammadex_rocuronium.RmdModel and source
- Citation: Kleijn HJ, Zollinger DP, van den Heuvel MW, Kerbusch T. Population pharmacokinetic-pharmacodynamic analysis for sugammadex-mediated reversal of rocuronium-induced neuromuscular blockade. Br J Clin Pharmacol. 2011 Sep;72(3):415-433. doi:10.1111/j.1365-2125.2011.04000.x. PMID: 21501216. Complex-formation framework from Bom AHJ, Bradley M, Cameron K, Clark JK, Van Egmond J, Feilden H, MacLean EJ, Muir AW, Palin R, Rees DC, Zhang MQ. A novel concept of reversing neuromuscular block: chemical encapsulation of rocuronium bromide by a cyclodextrin-based synthetic host. Angew Chem Int Ed Engl. 2002.
- Description: Integrated population PK-PD model for sugammadex-mediated reversal of rocuronium-induced neuromuscular blockade (Kleijn 2011). Both sugammadex and rocuronium have two-compartment PK from IV bolus dosing into the central compartment; the sugammadex-rocuronium inclusion complex has its own two-compartment PK with parameters set equal to free sugammadex (Bom 2002 framework). Complex formation is dynamic with fixed equilibrium dissociation constant kd = 0.0559 uM and estimated dissociation rate k2 = 0.034 1/min (association k1 = k2 / kd = 0.61 1/(minuM)). The rocuronium central concentration drives an effect compartment via ke0 = 0.134 1/min; neuromuscular blockade (T4/T1 twitch ratio x 100) follows a sigmoid Emax form with Emax set equal to E0 so the readout decreases monotonically from baseline E0 ~ 104 toward 0 as the effect-compartment rocuronium concentration rises. Sugammadex-mediated reversal enters as an additional first-order elimination of rocuronium from the effect compartment driven by the central free-sugammadex concentration (ks = 0.033 1/(minuM)). Both plasma assays measured total drug (free + complex), so the Cc and Cc_roc outputs return total sugammadex and total rocuronium. Allometric scaling on all volumes (exponent 1), flows (0.75), and rate constants (-0.25) at reference WT = 70 kg; sugammadex CL is NOT allometrically scaled (creatinine-clearance covariate replaces size scaling). All units are molar inside the model (dose in umol, concentrations in uM); see vignette for mg-to-umol conversion with rocuronium MW = 529.78 g/mol and sugammadex MW = 2178.01 g/mol (octasodium salt).
- Article: https://doi.org/10.1111/j.1365-2125.2011.04000.x
Population
The Kleijn 2011 cohort pooled 446 subjects across eight clinical
trials of sugammadex-mediated reversal of rocuronium-induced
neuromuscular blockade (NMB): healthy male volunteers, adult patients
undergoing general anaesthesia, a Japanese vs Caucasian sub-cohort,
renally impaired adults, elderly patients, and a paediatric cohort
spanning infants through adolescents (Table 1 of the paper). Age ranged
from 1 to 91 years (median 43), body weight from 9.60 to 139 kg (median
74.5), and creatinine clearance from 4.3 to 239 mL/min (median 119). 53
of 446 subjects were Asian (study 19.4.208 Part A; primarily Japanese).
Rocuronium IV bolus doses spanned 0.6 to 1.2 mg/kg; sugammadex IV bolus
doses spanned 0.1 to 16 mg/kg (with placebo arms in some studies).
Sugammadex was given either at a fixed time (3 min, 5 min, 15 min) after
rocuronium or at reappearance of T2 in the train-of-four. The same
metadata are available programmatically via
readModelDb("Kleijn_2011_sugammadex_rocuronium")$population.
Source trace
Per-parameter origin is recorded as an in-file comment alongside
every ini() entry in
inst/modeldb/specificDrugs/Kleijn_2011_sugammadex_rocuronium.R.
The table below consolidates these for review. All values come from
Kleijn 2011 Table 4 (the final integrated PK-PD model column).
| Equation / parameter | Value | Source location |
|---|---|---|
| Sugammadex CL (CRCL = 119 mL/min, BW = 74.5 kg) | 0.093 L/min | Table 4 sugammadex, CL |
| Sugammadex V1 (BW = 70 kg, non-Asian) | 4.42 L | Table 4 sugammadex, V1 |
| Sugammadex Q2 (BW = 70 kg) | 0.206 L/min | Table 4 sugammadex, Q2 |
| Sugammadex V2 (BW = 70 kg, CRCL = 119 mL/min) | 6.35 L | Table 4 sugammadex, V2 |
| Sugammadex CL renal-function exponent | 1.29 | Table 4 sugammadex, REN power exponent |
| Sugammadex CL BW slope (per kg from 74.5) | 0.00378 | Table 4 sugammadex, CL_BW |
| Sugammadex V1 BW slope (per kg from 74.5) | -0.00354 | Table 4 sugammadex, V1_BW |
| Sugammadex V1 Asian effect | -0.16 | Table 4 sugammadex, V1_RAC (Asian) |
| Sugammadex V2 CRCL slope (per mL/min from 119) | -0.00305 | Table 4 sugammadex, V2_CR |
| Rocuronium CL (AGE = 43 y, BW = 70 kg) | 0.269 L/min | Table 4 rocuronium, CL |
| Rocuronium V1 (BW = 70 kg, CRCL = 119 mL/min) | 4.73 L | Table 4 rocuronium, V1 |
| Rocuronium Q2 (BW = 70 kg, non-Asian) | 0.279 L/min | Table 4 rocuronium, Q2 |
| Rocuronium V2 (BW = 70 kg, AGE = 43 y) | 6.76 L | Table 4 rocuronium, V2 |
| Rocuronium CL AGE slope (per year from 43) | -0.00678 | Table 4 rocuronium, CL_AGE |
| Rocuronium V1 CRCL slope (per mL/min from 119) | -0.00143 | Table 4 rocuronium, V1_CR |
| Rocuronium Q2 Asian effect | -0.212 | Table 4 rocuronium, Q2_RAC (Asian) |
| Rocuronium V2 AGE slope (per year from 43) | 0.00613 | Table 4 rocuronium, V2_AGE |
| Complex equilibrium dissociation kd (FIXED) | 0.0559 uM | Table 4 complex, kd; Bom 2002 in vitro |
| Complex dissociation log_e(k2) | -3.38 (k2 = 0.034 1/min) | Table 4 complex, log_e(k2) |
| Rocuronium effect-cmt keo | 0.134 1/min | Table 4 rocuronium PD, keo |
| Sevoflurane multiplicative effect on keo | -0.567 | Table 4 rocuronium PD, keo_SEV |
| Rocuronium NMB EC50 | 1.62 uM | Table 4 rocuronium PD, EC50 |
| Sevoflurane multiplicative effect on EC50 | -0.395 | Table 4 rocuronium PD, EC50_SEV |
| Hill exponent of NMB sigmoid | 7.52 | Table 4 rocuronium PD, Hill |
| Typical T4/T1 x 100 baseline E0 | 104 (theta = 1.04, x 100) | Table 4 rocuronium PD, E0 |
| Sugammadex-mediated reversal log_e(ks) | -3.43 (ks = 0.033 1/(min*uM)) | Table 4 sugammadex PD, log_e(ks) |
| IIV CL sugammadex | 22.4% CV | Table 4 sugammadex, IIV CL |
| IIV CL / V1 / V2 rocuronium | 32.4 / 23.8 / 32.2% CV | Table 4 rocuronium, IIV CL / V1 / V2 |
| IIV keo / EC50 rocuronium (with r = 0.37) | 41.7 / 24.9% CV | Table 4 rocuronium PD, IIV keo / EC50; r = 0.37 |
| IIV Hill / E0 rocuronium | 41.1 / 11.1% CV | Table 4 rocuronium PD, IIV Hill / E0 |
| IIV ks sugammadex | 114% CV | Table 4 sugammadex PD, IIV ks |
| Proportional residual on sugammadex Cc | 36.3% | Table 4 sugammadex, residual error (log-additive) |
| Proportional residual on rocuronium Cc | 20.0% | Table 4 rocuronium, residual error (log-additive) |
| Additive residual on NMB (T4/T1 x 100) | 3.24 | Table 4 sugammadex PD, residual error (T4/T1 x 100) |
| Allometric exponents on V, CL, rate constants | 1, 0.75, -0.25 (FIXED) | Methods, “Size effects” |
| Sugammadex CL NOT allometrically scaled | n/a | Methods, “Renal function” |
| Two-compartment PK for sug, roc, complex | n/a | Methods, “Pharmacokinetic model development” |
| Complex PK = sugammadex PK | n/a | Methods, “Pharmacokinetic model development” |
| Sigmoid Emax NMB with Emax = E0 | n/a | Methods, “PK-PD model development” |
| Sugammadex reversal via ks on effect_roc | n/a | Methods, “PK-PD model development” |
| Cc and Cc_roc = free + complex (total) | n/a | Methods, “Rocuronium and sugammadex plasma concs.” |
Virtual cohort
Original observed data are not publicly available. The virtual subjects below mirror the five typical-subject definitions in Kleijn 2011 Table 3 (infant 1 year, child 7 years, adolescent 15 years, adult 40 years, elderly 75 years) at normal renal function. Doses are converted from mg to umol using the molecular weights rocuronium MW = 529.78 g/mol and sugammadex sodium MW = 2178.01 g/mol.
MW_ROC <- 529.78 # g/mol
MW_SUG <- 2178.01 # g/mol (octasodium salt; the form used in clinical product)
# Per-paper typical subjects (Table 3). RACE_ASIAN = 0 throughout.
typical <- tibble::tribble(
~cohort, ~WT, ~AGE, ~CRCL, ~RACE_ASIAN, ~CONMED_SEVO,
"Infant 1 y", 10.3, 1, 25.7, 0, 0,
"Child 7 y", 23.0, 7, 51.2, 0, 0,
"Adolescent 15 y", 56.2, 15, 95.3, 0, 0,
"Adult 40 y", 75.0, 40, 100, 0, 0,
"Elderly 75 y", 75.0, 75, 80, 0, 0
)
knitr::kable(typical, caption = "Typical subjects from Kleijn 2011 Table 3 (normal renal function row).")| cohort | WT | AGE | CRCL | RACE_ASIAN | CONMED_SEVO |
|---|---|---|---|---|---|
| Infant 1 y | 10.3 | 1 | 25.7 | 0 | 0 |
| Child 7 y | 23.0 | 7 | 51.2 | 0 | 0 |
| Adolescent 15 y | 56.2 | 15 | 95.3 | 0 | 0 |
| Adult 40 y | 75.0 | 40 | 100.0 | 0 | 0 |
| Elderly 75 y | 75.0 | 75 | 80.0 | 0 | 0 |
Simulation
mod <- readModelDb("Kleijn_2011_sugammadex_rocuronium")
mod_typical <- rxode2::zeroRe(mod)
#> ℹ parameter labels from comments will be replaced by 'label()'We simulate three canonical reversal scenarios per typical subject:
- Immediate reversal: rocuronium 1.2 mg/kg at t = 0, sugammadex 16 mg/kg at t = 3 min.
- Deep blockade reversal: rocuronium 0.6 mg/kg at t = 0, sugammadex 4 mg/kg at t = 15 min.
- Moderate blockade reversal: rocuronium 0.6 mg/kg at t = 0, sugammadex 2 mg/kg at the model-predicted T2 reappearance.
Reversal time is the time from the sugammadex dose to recovery of NMB to 90 (TOF90) or 70 (TOF70) on the T4/T1 x 100 scale.
# Helper: build event table for one subject and one scenario. When
# sug_mgkg == 0 (spontaneous-recovery scenario) the sugammadex dose row
# is omitted entirely.
make_events <- function(WT, AGE, CRCL, RACE_ASIAN, CONMED_SEVO,
roc_mgkg, sug_mgkg, t_sug,
t_end, dt = 0.1) {
amt_roc <- WT * roc_mgkg / MW_ROC * 1000 # umol
obs_times <- seq(0, t_end, by = dt)
if (sug_mgkg > 0) {
amt_sug <- WT * sug_mgkg / MW_SUG * 1000 # umol
dose_rows <- tibble::tibble(
id = 1L,
time = c(0, t_sug),
evid = c(1L, 1L),
amt = c(amt_roc, amt_sug),
cmt = c("central_roc", "central")
)
} else {
dose_rows <- tibble::tibble(
id = 1L, time = 0, evid = 1L,
amt = amt_roc, cmt = "central_roc"
)
}
obs_rows <- tibble::tibble(
id = 1L, time = obs_times, evid = 0L, amt = 0,
cmt = "NMB"
)
ev <- dplyr::bind_rows(dose_rows, obs_rows) |>
dplyr::arrange(id, time, evid)
ev$WT <- WT; ev$AGE <- AGE; ev$CRCL <- CRCL
ev$RACE_ASIAN <- RACE_ASIAN; ev$CONMED_SEVO <- CONMED_SEVO
ev
}
# Helper: compute reversal time from a sim trace.
reversal_time <- function(sim_df, t_sug, target_nmb) {
post <- sim_df |> dplyr::filter(time >= t_sug)
hit <- which(post$NMB >= target_nmb)
if (length(hit) == 0) return(NA_real_)
post$time[hit[1]] - t_sug
}
# Find T2 reappearance: first time after the rocuronium-induced deep
# block (NMB < 1) that NMB rises above 1 again. Using NMB = 1 on the
# 0-100 scale as a proxy: the train-of-four T2 first becomes detectable
# when the block lifts above zero. We require that NMB has BEEN below 1
# (i.e., the deep block established) before counting the upward
# crossing as "reappearance".
t2_reappearance <- function(sim_df) {
# Skip the baseline (NMB ~ E0) by waiting for NMB to drop below 1
# first, then finding the next upward crossing of 1.
was_blocked <- sim_df$NMB < 1
if (!any(was_blocked)) return(NA_real_)
first_block <- which(was_blocked)[1]
recovery_idx <- which(sim_df$NMB >= 1 & seq_along(sim_df$NMB) > first_block)
if (length(recovery_idx) == 0) return(NA_real_)
sim_df$time[recovery_idx[1]]
}
results <- list()
sim_traces <- list()
for (i in seq_len(nrow(typical))) {
s <- typical[i, ]
# Scenario 1: Immediate reversal (1.2 mg/kg roc, 16 mg/kg sug at 3 min)
ev1 <- make_events(s$WT, s$AGE, s$CRCL, s$RACE_ASIAN, s$CONMED_SEVO,
roc_mgkg = 1.2, sug_mgkg = 16, t_sug = 3, t_end = 60)
sim1 <- as.data.frame(rxode2::rxSolve(mod_typical, ev1))
t90_1 <- reversal_time(sim1, 3, 90)
# Scenario 2: Deep blockade reversal (0.6 mg/kg roc, 4 mg/kg sug at 15 min)
ev2 <- make_events(s$WT, s$AGE, s$CRCL, s$RACE_ASIAN, s$CONMED_SEVO,
roc_mgkg = 0.6, sug_mgkg = 4, t_sug = 15, t_end = 80)
sim2 <- as.data.frame(rxode2::rxSolve(mod_typical, ev2))
t90_2 <- reversal_time(sim2, 15, 90)
# Scenario 3: Moderate blockade reversal (0.6 mg/kg roc, sug 2 mg/kg at
# T2 reappearance). First find T2 reappearance under spontaneous
# recovery, then re-simulate with sug at that time.
ev3_spontaneous <- make_events(s$WT, s$AGE, s$CRCL, s$RACE_ASIAN, s$CONMED_SEVO,
roc_mgkg = 0.6, sug_mgkg = 0,
t_sug = 0, t_end = 200)
sim3_spont <- as.data.frame(rxode2::rxSolve(mod_typical, ev3_spontaneous))
t_T2 <- t2_reappearance(sim3_spont)
ev3 <- make_events(s$WT, s$AGE, s$CRCL, s$RACE_ASIAN, s$CONMED_SEVO,
roc_mgkg = 0.6, sug_mgkg = 2, t_sug = t_T2,
t_end = t_T2 + 30)
sim3 <- as.data.frame(rxode2::rxSolve(mod_typical, ev3))
t90_3 <- reversal_time(sim3, t_T2, 90)
results[[i]] <- data.frame(
cohort = s$cohort,
`Immediate (16 mg/kg)` = t90_1,
`Deep (4 mg/kg)` = t90_2,
`Moderate (2 mg/kg, at T2)` = t90_3,
check.names = FALSE
)
sim_traces[[paste0(s$cohort, "_immediate")]] <- dplyr::mutate(sim1, scenario = "Immediate", cohort = s$cohort, t_sug = 3)
sim_traces[[paste0(s$cohort, "_deep")]] <- dplyr::mutate(sim2, scenario = "Deep blockade", cohort = s$cohort, t_sug = 15)
sim_traces[[paste0(s$cohort, "_moderate")]] <- dplyr::mutate(sim3, scenario = "Moderate blockade", cohort = s$cohort, t_sug = t_T2)
}
reversal_table <- dplyr::bind_rows(results) |>
dplyr::mutate(dplyr::across(-cohort, ~ round(.x, 2)))
knitr::kable(reversal_table,
caption = "Simulated reversal times (min) to TOF90 for typical subjects (Kleijn 2011 Table 6, normal renal function, no sevoflurane).")| cohort | Immediate (16 mg/kg) | Deep (4 mg/kg) | Moderate (2 mg/kg, at T2) |
|---|---|---|---|
| Infant 1 y | 0.6 | 0.8 | 1.3 |
| Child 7 y | 0.6 | 1.2 | 1.5 |
| Adolescent 15 y | 0.7 | 1.6 | 1.7 |
| Adult 40 y | 0.7 | 1.8 | 1.8 |
| Elderly 75 y | 0.7 | 2.0 | 1.8 |
Replicate published figures
Figure 5 style: rocuronium NMB recovery profiles (no sugammadex)
The next chunk plots spontaneous T4/T1 recovery after rocuronium 0.6 mg/kg or 1.2 mg/kg (no sugammadex) for the adult 40 y typical subject, with and without sevoflurane. This mirrors the upper panels of Figure 5 of the paper.
fig5_scenarios <- tibble::tribble(
~label, ~roc_mgkg, ~CONMED_SEVO,
"0.6 mg/kg roc, no sevoflurane", 0.6, 0,
"1.2 mg/kg roc, no sevoflurane", 1.2, 0,
"0.6 mg/kg roc, sevoflurane", 0.6, 1
)
adult <- typical[typical$cohort == "Adult 40 y", ]
fig5_data <- purrr::map_dfr(seq_len(nrow(fig5_scenarios)), function(k) {
r <- fig5_scenarios[k, ]
ev <- make_events(adult$WT, adult$AGE, adult$CRCL, adult$RACE_ASIAN, r$CONMED_SEVO,
roc_mgkg = r$roc_mgkg, sug_mgkg = 0, t_sug = 0,
t_end = 200, dt = 1)
sim <- as.data.frame(rxode2::rxSolve(mod_typical, ev))
dplyr::mutate(sim, scenario = r$label)
})
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
ggplot(fig5_data, aes(time, NMB, colour = scenario)) +
geom_line() +
geom_hline(yintercept = c(70, 90), linetype = "dashed", colour = "grey50") +
labs(x = "Time after rocuronium dose (min)",
y = "T4/T1 twitch ratio x 100",
title = "Figure 5 (style): spontaneous rocuronium NMB recovery",
caption = "Replicates upper panels of Figure 5 of Kleijn 2011 (T4/T1 vs. time after rocuronium).")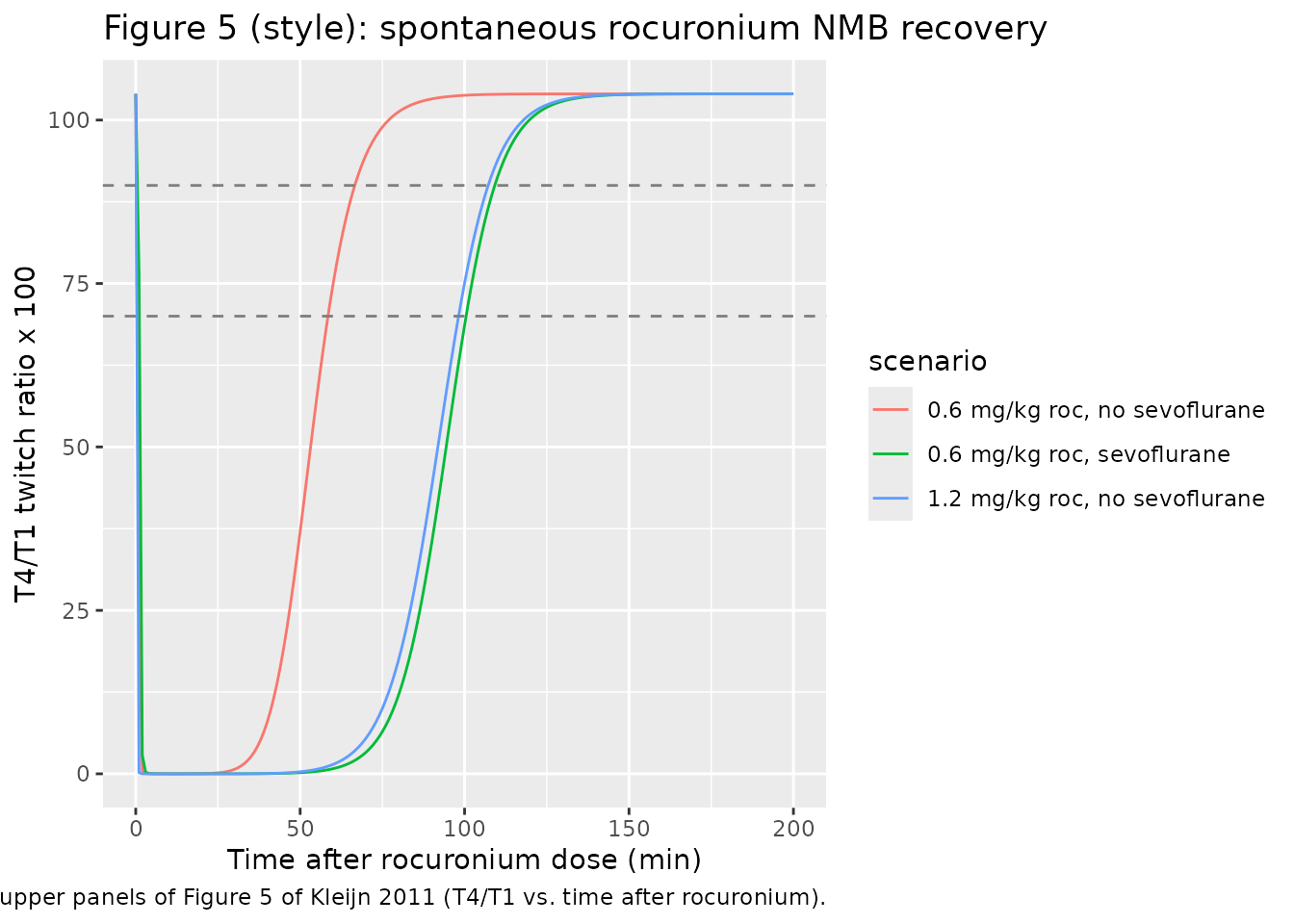
Table 6 style: reversal-time cross-tabulation
The reversal_table above reproduces the structure of Kleijn 2011 Table 6 (typical reversal times by age cohort and scenario, normal renal function, non-Asian, no sevoflurane). The paper’s published medians for the adult 40-year reference cohort are:
- Immediate reversal (16 mg/kg sug at 3 min after 1.2 mg/kg roc): 0.8 min
- Deep blockade reversal (4 mg/kg sug at 15 min after 0.6 mg/kg roc): 1.5 min
- Moderate blockade reversal (2 mg/kg sug at T2 reappearance): 1.4 min
Simulated typical-subject reversal times should be close to these (within the simulated time-step resolution and the t2_reappearance proxy used for the moderate scenario). Larger discrepancies in the simulated TOF90 for the moderate scenario reflect the difference between the paper’s T2-reappearance trigger (the train-of-four T2 first becoming visible on accelerography) and our NMB-rises-above-1 proxy; both are first-recovery markers but their exact timing differs.
Sugammadex plasma profile (Figure 2 style)
adult <- typical[typical$cohort == "Adult 40 y", ]
sug_doses_mgkg <- c(0.5, 1, 2, 4, 8, 16)
fig2 <- purrr::map_dfr(sug_doses_mgkg, function(d) {
ev <- make_events(adult$WT, adult$AGE, adult$CRCL, adult$RACE_ASIAN, adult$CONMED_SEVO,
roc_mgkg = 0.6, sug_mgkg = d, t_sug = 15, t_end = 600,
dt = 1)
# Add observations for Cc as well (re-route to Cc cmt)
obs_cc <- tibble::tibble(id = 1L,
time = seq(15, 600, by = 1),
evid = 0L, amt = 0, cmt = "Cc",
WT = adult$WT, AGE = adult$AGE, CRCL = adult$CRCL,
RACE_ASIAN = adult$RACE_ASIAN, CONMED_SEVO = adult$CONMED_SEVO)
ev2 <- dplyr::bind_rows(ev, obs_cc) |> dplyr::arrange(id, time, evid)
sim <- as.data.frame(rxode2::rxSolve(mod_typical, ev2))
sim |>
dplyr::filter(time >= 15) |>
dplyr::mutate(dose_mgkg = d,
t_post_sug = time - 15,
# Convert uM to ug/mL for plotting (uM * MW / 1000)
Cc_ugmL = Cc * MW_SUG / 1000)
})
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
# Plot sugammadex plasma concentration (total = free + complex) by dose.
ggplot(fig2 |> dplyr::filter(t_post_sug > 0), aes(t_post_sug, Cc_ugmL, colour = factor(dose_mgkg))) +
geom_line() +
scale_y_log10() +
labs(x = "Time after sugammadex dose (min)",
y = "Total sugammadex (ug/mL)",
colour = "Dose (mg/kg)",
title = "Figure 2 (style): typical adult sugammadex plasma profile",
caption = "Replicates the typical-value panel of Figure 2 of Kleijn 2011.")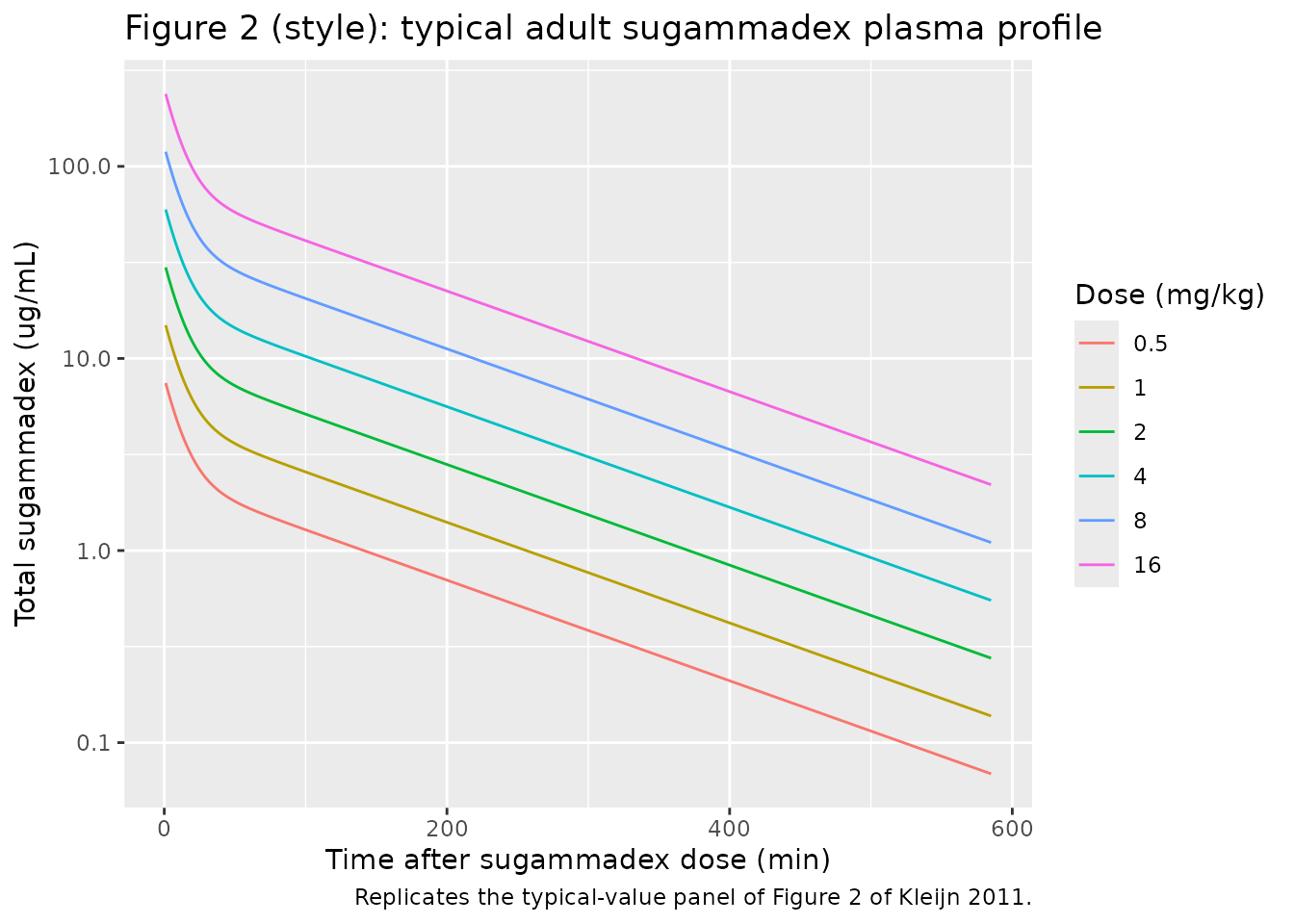
PKNCA validation
We compute non-compartmental Cmax, Tmax, AUC0-inf, and t1/2 for a typical adult given a sugammadex 4 mg/kg IV bolus (no rocuronium) and a separate rocuronium 0.6 mg/kg IV bolus (no sugammadex). Without the complex-formation pathway, the model reduces to two independent 2-compartment IV-bolus PK subsystems, and the simulated NCA parameters should match the analytical values derived from the structural parameters.
adult <- typical[typical$cohort == "Adult 40 y", ]
amt_sug <- adult$WT * 4 / MW_SUG * 1000 # umol from 4 mg/kg
# Sugammadex-only event table with explicit time-zero Cc record so PKNCA
# does not warn about an AUC range starting before the first measurement.
times_sug <- c(0, seq(0.1, 1, by = 0.1), seq(2, 30, by = 1),
seq(40, 240, by = 10), seq(300, 1440, by = 60))
ev_sug <- dplyr::bind_rows(
tibble::tibble(id = 1L, time = 0, evid = 1L, amt = amt_sug, cmt = "central"),
tibble::tibble(id = 1L, time = times_sug, evid = 0L, amt = 0, cmt = "Cc")
)
ev_sug$WT <- adult$WT; ev_sug$AGE <- adult$AGE
ev_sug$CRCL <- adult$CRCL; ev_sug$RACE_ASIAN <- adult$RACE_ASIAN
ev_sug$CONMED_SEVO <- adult$CONMED_SEVO
sim_sug <- as.data.frame(rxode2::rxSolve(mod_typical, ev_sug))
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
conc_sug <- sim_sug |>
dplyr::filter(!is.na(Cc)) |>
dplyr::transmute(id = 1L, time = time,
Cc_ugmL = Cc * MW_SUG / 1000)
dose_df_sug <- tibble::tibble(id = 1L, time = 0,
amt = adult$WT * 4) # mg
pknca_sug <- PKNCA::pk.nca(PKNCA::PKNCAdata(
PKNCA::PKNCAconc(conc_sug, Cc_ugmL ~ time | id),
PKNCA::PKNCAdose(dose_df_sug, amt ~ time | id),
intervals = data.frame(start = 0, end = Inf,
cmax = TRUE, tmax = TRUE,
aucinf.obs = TRUE, half.life = TRUE)
))
nca_sug_df <- as.data.frame(pknca_sug$result) |>
dplyr::select(PPTESTCD, PPORRES) |>
dplyr::mutate(PPORRES = signif(PPORRES, 4))
knitr::kable(nca_sug_df,
caption = "Simulated sugammadex NCA for adult 40 y, 4 mg/kg IV bolus.")| PPTESTCD | PPORRES |
|---|---|
| cmax | 6.346e+01 |
| tmax | 0.000e+00 |
| tlast | 1.440e+03 |
| clast.obs | 3.173e-03 |
| lambda.z | 6.039e-03 |
| r.squared | 1.000e+00 |
| adj.r.squared | 1.000e+00 |
| lambda.z.time.first | 4.000e+01 |
| lambda.z.time.last | 1.440e+03 |
| lambda.z.n.points | 4.100e+01 |
| clast.pred | 3.159e-03 |
| half.life | 1.148e+02 |
| span.ratio | 1.220e+01 |
| aucinf.obs | 3.622e+03 |
amt_roc <- adult$WT * 0.6 / MW_ROC * 1000 # umol from 0.6 mg/kg
times_roc <- c(0, seq(0.1, 1, by = 0.1), seq(2, 30, by = 1),
seq(40, 240, by = 10))
ev_roc <- dplyr::bind_rows(
tibble::tibble(id = 1L, time = 0, evid = 1L, amt = amt_roc, cmt = "central_roc"),
tibble::tibble(id = 1L, time = times_roc, evid = 0L, amt = 0, cmt = "Cc_roc")
)
ev_roc$WT <- adult$WT; ev_roc$AGE <- adult$AGE
ev_roc$CRCL <- adult$CRCL; ev_roc$RACE_ASIAN <- adult$RACE_ASIAN
ev_roc$CONMED_SEVO <- adult$CONMED_SEVO
sim_roc <- as.data.frame(rxode2::rxSolve(mod_typical, ev_roc))
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalcl_roc', 'etalvc_roc', 'etalvp_roc', 'etalke0', 'etalec50', 'etalhill', 'etale0', 'etalks'
conc_roc <- sim_roc |>
dplyr::filter(!is.na(Cc_roc)) |>
dplyr::transmute(id = 1L, time = time,
Cc_roc_ngmL = Cc_roc * MW_ROC) # uM -> ng/mL
dose_df_roc <- tibble::tibble(id = 1L, time = 0,
amt = adult$WT * 0.6) # mg
pknca_roc <- PKNCA::pk.nca(PKNCA::PKNCAdata(
PKNCA::PKNCAconc(conc_roc, Cc_roc_ngmL ~ time | id),
PKNCA::PKNCAdose(dose_df_roc, amt ~ time | id),
intervals = data.frame(start = 0, end = Inf,
cmax = TRUE, tmax = TRUE,
aucinf.obs = TRUE, half.life = TRUE)
))
nca_roc_df <- as.data.frame(pknca_roc$result) |>
dplyr::select(PPTESTCD, PPORRES) |>
dplyr::mutate(PPORRES = signif(PPORRES, 4))
knitr::kable(nca_roc_df,
caption = "Simulated rocuronium NCA for adult 40 y, 0.6 mg/kg IV bolus.")| PPTESTCD | PPORRES |
|---|---|
| cmax | 8.641e+03 |
| tmax | 0.000e+00 |
| tlast | 2.400e+02 |
| clast.obs | 3.133e+01 |
| lambda.z | 1.687e-02 |
| r.squared | 1.000e+00 |
| adj.r.squared | 1.000e+00 |
| lambda.z.time.first | 4.000e+01 |
| lambda.z.time.last | 2.400e+02 |
| lambda.z.n.points | 2.100e+01 |
| clast.pred | 3.122e+01 |
| half.life | 4.110e+01 |
| span.ratio | 4.867e+00 |
| aucinf.obs | 1.558e+05 |
Comparison against published values
The paper does not tabulate per-subject NCA, but several derived quantities are reported in the Results / Discussion:
- Sugammadex elimination half-life in plasma is reported as ~ 2 h (120 min) in healthy subjects (Discussion); rises to ~ 20 h (1200 min) in severe renal impairment.
- Rocuronium effect-compartment half-life at baseline (no sugammadex) is log(2) / keo = log(2) / 0.134 = 5.17 min (Methods, “PK-PD analysis”).
- Rocuronium effect-compartment half-life with 4 mg/kg sugammadex is reported as 0.71 min immediately after the dose (Methods: “Immediately after administration of sugammadex 2 or 4 mg/kg, the rocuronium elimination half-life from the effect compartment was calculated to be 1.43 and 0.71 min, respectively”).
- Complex association / dissociation half-lives: 1.1 min and 20.4 min respectively (Results).
The simulated sugammadex t1/2 (from PKNCA above) should be on the order of 60-120 min for the normal-renal-function adult. The simulated rocuronium NCA t1/2 should be on the order of 60-90 min (terminal elimination phase, in the absence of sugammadex).
Assumptions and deviations
-
All units are molar inside the model.
Concentrations are in uM (umol/L); doses must be supplied in umol. The
vignette converts mg-doses to umol using rocuronium MW = 529.78 g/mol
and sugammadex MW = 2178.01 g/mol (the octasodium salt form used in the
marketed product). Users who prefer to dose in mg should add an
f(central) <- 1 / MW_SUG * 1000and similar bioavailability factors at the model layer, or pre-convert at the event-table layer (as we do here). - Sugammadex CL is NOT allometrically scaled by body weight (in contrast to all other PK parameters and rate constants). Kleijn 2011 Methods, “Renal function”: “As size effects were already included in creatinine clearance, clearance of sugammadex was not allometrically scaled”.
- Allometric exponents are FIXED at 0.75 / 1 / -0.25 (Methods, “Size effects”). Not estimated.
- kd is FIXED at 0.0559 uM from in-vitro (Methods, citing Bom 2002); only the dissociation rate k2 is estimated. The association rate is derived as k1 = k2 / kd = 0.61 1/(min*uM).
-
The complex has its own PK (= sugammadex PK) – not
separately estimated. The dosing into
central_complexis zero; the compartment is populated only by the complexation flux. -
Total drug = free + complex in the assay (Methods,
“Rocuronium and sugammadex plasma concentrations”);
CcandCc_roctherefore return total drug. - Sugammadex-mediated reversal acts on the effect compartment, not on the central rocuronium compartment (Methods, “PK-PD model development”). The mass balance is therefore not strictly conservative for free rocuronium (some “rocuronium” leaves the effect compartment without returning to central), but this is a faithful reproduction of the paper’s mechanistic abstraction: ks represents sugammadex consumption of rocuronium at the neuromuscular-junction site of action.
-
NMB readout is on the T4/T1 x 100 scale. Baseline
E0is ~ 104; full block reaches ~ 0. Reversal-time endpoints TOF90 (recovery to 90) and TOF70 (recovery to 70) are read off the simulated trace as the first time after the sugammadex dose at which NMB rises above the target. -
Two PD residual errors are reported in the paper
(2.70 from the rocuronium-PD fit on placebo patients; 3.24 from the
sugammadex-PD fit on combined data). The model uses 3.24 (the larger
combined-data residual) as
addSd_NMBbecause the primary use of this library is forward simulation of reversal scenarios under both drugs; the rocuronium-only residual 2.70 is documented in the source-trace comment. -
Sevoflurane is encoded as a binary indicator
CONMED_SEVO, in line with the paper’s per-subject treatment of “sevoflurane anaesthesia used”. An end-tidal-concentration-driven continuous model (Shin 2014 style, via the canonicalETSEVOcovariate) would require time-resolved sevoflurane concentrations that Kleijn 2011 did not collect. -
Race is a binary Asian-vs-non-Asian indicator
(
RACE_ASIAN). The paper’s Asian sub-cohort came primarily from study 19.4.208 Part A (Japanese subjects); the same fixed effect would apply to any subject marked RACE_ASIAN = 1. - Reversal-time simulations use a typical-subject proxy for T2 reappearance (the first time after rocuronium that NMB rises above 1 on the 0-100 scale). The paper’s external-validation simulations used a matched dosing schedule taken from the trial; we use the model-predicted T2 reappearance because the underlying trial-by-trial dosing data are not publicly available.