Model and source
- Citation: Chae JW, Baek IH, Lee BY, Cho SK, Kwon KI. Population pharmacokinetic and pharmacodynamic analysis of metformin using the signal transduction model. Br J Clin Pharmacol. 2012;74(5):815-823. doi:10.1111/j.1365-2125.2012.04260.x
- Description: One-compartment population PK model with first-order absorption for oral metformin in healthy Korean adults, coupled to a three-transit Sun-Jusko signal-transduction PD model for the antihyperglycaemic effect (Chae 2012). Plasma drug concentration in the central compartment drives a Hill-type stimulation function DR = Emax * Cp^r / (EC50^r + Cp^r) that initiates a cascade of three secondary-messenger transit compartments (M1 -> M2 -> M3) with shared mean transit time tau. The third messenger M3 is the measured percent change in plasma glucose from baseline relative to a sugar-bolus control arm. Creatinine clearance enters CL/F as a power covariate with reference 106.5 mL/min and exponent 0.782.
- Article: https://doi.org/10.1111/j.1365-2125.2012.04260.x
Population
Chae 2012 enrolled 42 healthy young Korean male volunteers (age 21-31
years, weight 61-78 kg, baseline fasting plasma glucose 98 +/- 7 mg/dL,
creatinine clearance 90-123 mL/min) at a single centre in Daejeon. Each
subject received a single 500 mg oral metformin tablet (Diabex 500 mg,
Daewoong) after an overnight fast and consumed 12 g of sugar 20 min
after dosing. Identical sampling without metformin was performed one
week later to derive the antihyperglycaemic “percent-effect” PD endpoint
as the time-matched percent change in plasma glucose relative to the
no-metformin control arm. Per-subject demographics are Chae 2012 Table
1; the same information is available programmatically via
rxode2::rxode2(readModelDb("Chae_2012_metformin"))$population
after the model is loaded.
Source trace
Every parameter line in
inst/modeldb/specificDrugs/Chae_2012_metformin.R carries an
in-file source comment. The table below collects the equation and
parameter origins in one place for reviewer convenience.
| Equation / parameter | Value | Source location |
|---|---|---|
1-compartment PK ODEs dX1/dt = -Ka*X1,
dX2/dt = Ka*X1 - CL*X2/V2
|
n/a | Chae 2012 p.817 (Population PK/PD analysis) |
Signal-transduction PD:
DR = Emax*Cp^r / (EC50^r + Cp^r), transit chain
dMn/dt = (M_{n-1} - Mn)/tau, R = M3
|
n/a | Chae 2012 p.818 (Methods) and Figure 2 |
Ka (lka) |
0.41 1/h | Chae 2012 Table 2 (RSE 2.43%) |
CL/F (lcl) |
52.6 L/h | Chae 2012 Table 2 (RSE 4.18%); covariate equation p.819 |
V/F (lvc) |
113 L | Chae 2012 Table 2 (RSE 56.6%) |
CL/F covariate (CRCL/106.5)^0.782
(e_crcl_cl) |
0.782; ref 106.5 mL/min | Chae 2012 p.819 final-PK structural equation |
Mean transit time tau (ltau) |
0.50 h | Chae 2012 Table 2 (RSE 2.97%) |
Emax (lemax) |
19.8 (% effect) | Chae 2012 Table 2 (RSE 3.17%) |
EC50 (lec50) |
3.68 ug/mL | Chae 2012 Table 2 (RSE 3.89%) |
Hill r (lhill) |
0.55 | Chae 2012 Table 2 (RSE 9.05%) |
IIV CL 29.7% CV (etalcl ~ 0.08457) |
omega^2 = log(0.297^2 + 1) | Chae 2012 Table 2 (IIV CV% column) |
IIV V 22.1% CV (etalvc ~ 0.04769) |
omega^2 = log(0.221^2 + 1) | Chae 2012 Table 2 (IIV CV% column) |
IIV r 4.05% CV (etalhill ~ 0.001639) |
omega^2 = log(0.0405^2 + 1) | Chae 2012 Table 2 (IIV CV% column) |
| PK residual (additive, ng/mL -> ug/mL) | addSd = 0.023 |
Chae 2012 Table 2 (23 ng/mL, RSE 11.7%) |
| PD residual (proportional, fraction) | propSd_pctEffect = 0.404 |
Chae 2012 Table 2 (40.4%, RSE 1.52%) |
Virtual cohort
Original observed data from the 42-subject study are not publicly available. The figures below use a 200-subject virtual cohort whose covariate distributions approximate the published Korean-male healthy cohort (Chae 2012 Table 1) and whose sampling schedule matches the Chae 2012 study (0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10, 12 h post-dose, augmented with t = 0 and dense early sampling for PKNCA).
set.seed(20120815)
n_sub <- 200L
pop <- tibble(
ID = seq_len(n_sub),
AGE = round(runif(n_sub, 21, 31), 1),
WT = round(rnorm(n_sub, mean = 68.63, sd = 8.14), 1),
CRCL = pmax(80, pmin(130, round(rnorm(n_sub, mean = 106.5, sd = 16), 1))),
treatment = "500 mg PO"
)
# Dose records (single 500 mg oral dose into depot at t = 0)
d_dose <- pop |>
dplyr::mutate(TIME = 0, EVID = 1L, AMT = 500, CMT = "depot", DV = NA_real_)
# Observation records (sampling schedule covers absorption peak and terminal phase)
obs_times <- c(0, 0.25, 0.5, 1, 1.5, 2, 2.5, 3, 4, 6, 8, 10, 12)
d_obs <- pop[rep(seq_len(n_sub), each = length(obs_times)), ] |>
dplyr::mutate(
TIME = rep(obs_times, times = n_sub),
EVID = 0L,
AMT = 0,
CMT = "Cc",
DV = NA_real_
)
events <- dplyr::bind_rows(d_dose, d_obs) |>
dplyr::arrange(ID, TIME, dplyr::desc(EVID))
stopifnot(!anyDuplicated(unique(events[, c("ID", "TIME", "EVID")])))Simulation
mod <- rxode2::rxode2(readModelDb("Chae_2012_metformin"))
#> ℹ parameter labels from comments will be replaced by 'label()'
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("treatment", "WT", "AGE", "CRCL")
) |>
as.data.frame()Replicate published figures
Figure 5A – metformin concentration VPC
The packaged model reproduces the plasma-metformin VPC shape reported in Chae 2012 Figure 5A: rapid first-order absorption, Cmax around 1.5-1.8 ug/mL at Tmax ~= 2 h, monotonic decline to ~0.2 ug/mL by 12 h.
sim |>
dplyr::filter(time > 0) |>
group_by(time) |>
summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot(aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25, fill = "steelblue") +
geom_line(linewidth = 0.8) +
labs(
x = "Time after metformin dosing (h)",
y = "Metformin concentration (ug/mL)",
title = "Figure 5A replication -- metformin VPC (500 mg single oral dose)",
caption = "Median (line) and 5th/95th percentiles (band) from 200 virtual subjects."
)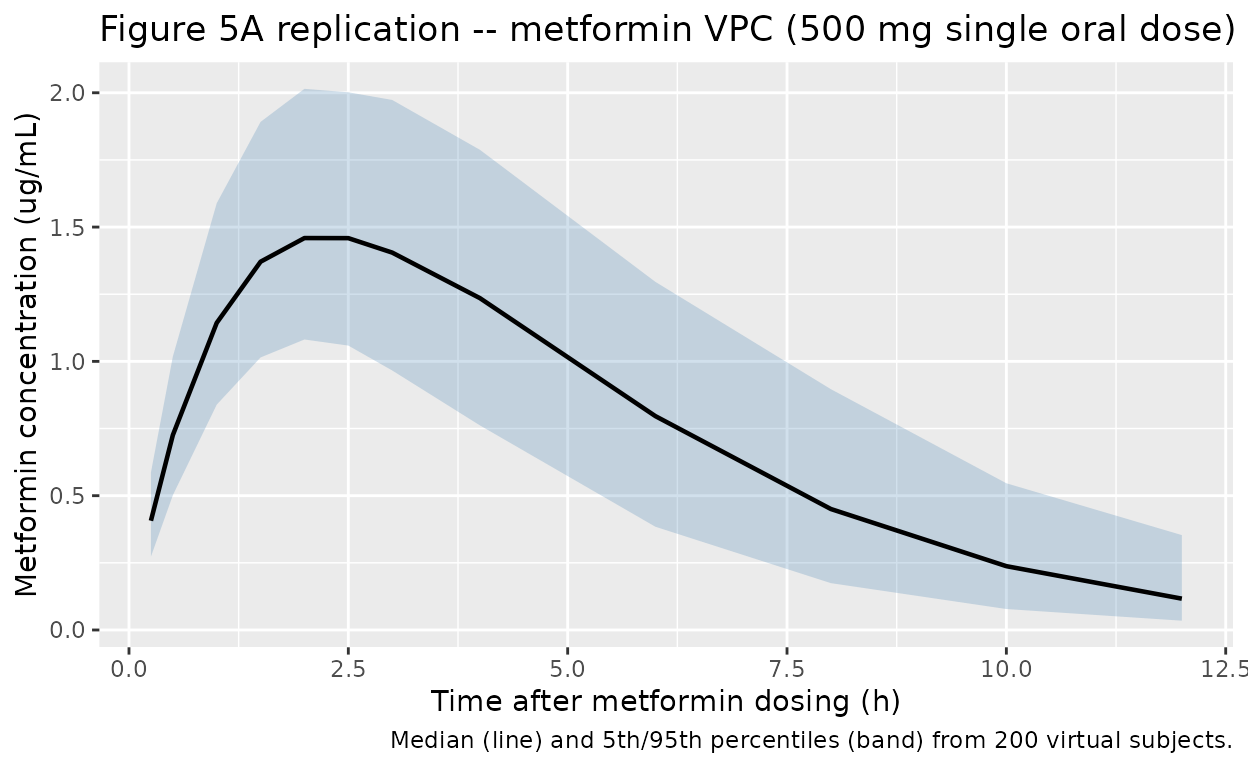
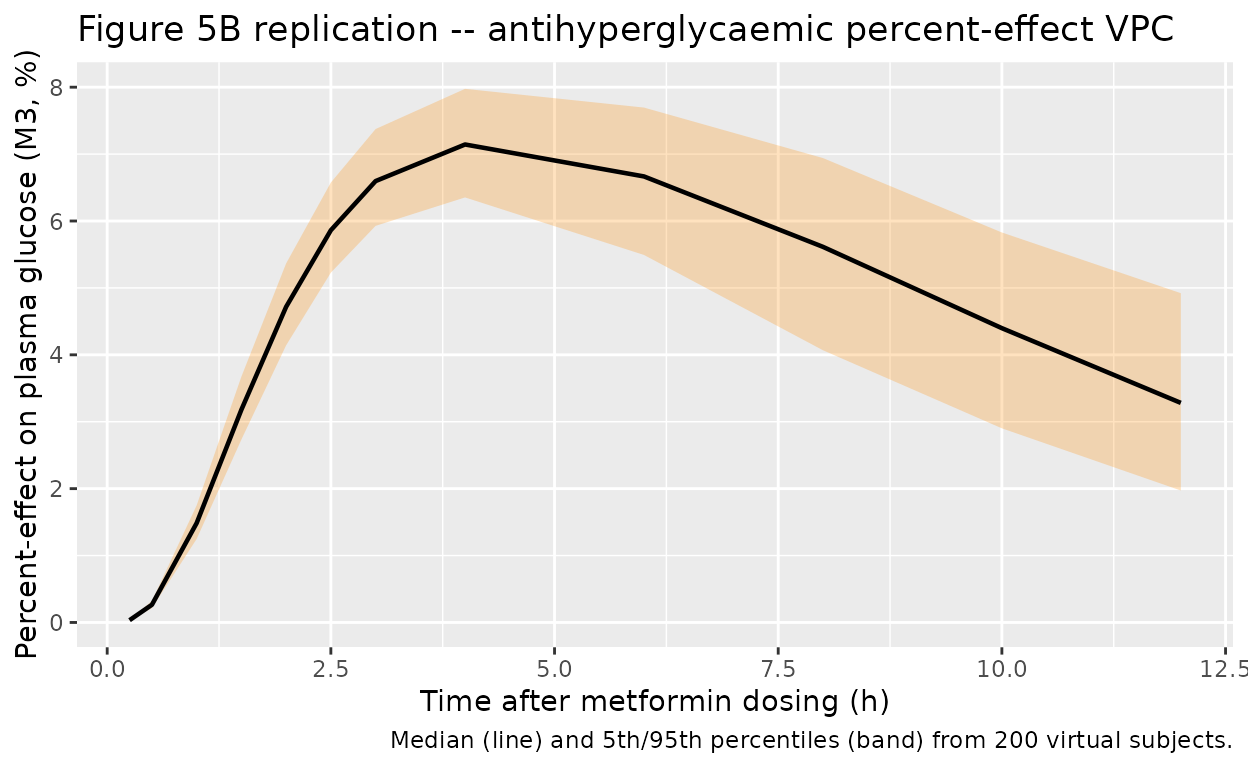
Figure 5B – antihyperglycaemic PD effect
Chae 2012 Figure 5B plots the absolute fasting plasma glucose
vs. time, while the structural PD model itself fits the percent-effect
endpoint R = M3 = pctEffect (percent change in plasma
glucose relative to the no-metformin sugar-bolus control arm). The plot
below shows the simulated percent-effect trajectory: a delayed onset
peaking around 3-4 h post-dose with a maximum of approximately Emax =
19.8% and a return toward baseline by 12 h, matching the FPG nadir
position in Chae 2012 Figure 5B (after accounting for the
back-conversion of percent effect to absolute glucose).
sim |>
dplyr::filter(time > 0) |>
group_by(time) |>
summarise(
Q05 = quantile(pctEffect, 0.05, na.rm = TRUE),
Q50 = quantile(pctEffect, 0.50, na.rm = TRUE),
Q95 = quantile(pctEffect, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot(aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25, fill = "darkorange") +
geom_line(linewidth = 0.8) +
labs(
x = "Time after metformin dosing (h)",
y = "Percent-effect on plasma glucose (M3, %)",
title = "Figure 5B replication -- antihyperglycaemic percent-effect VPC",
caption = "Median (line) and 5th/95th percentiles (band) from 200 virtual subjects."
)
PKNCA validation
Chae 2012 does not tabulate NCA parameters for the metformin PK profile (the paper validates the model through bootstrap-CI parameter estimation and a visual predictive check rather than a side-by-side NCA comparison). The NCA block below reports simulated Cmax, Tmax, AUC0-inf, and t1/2 from the packaged model as an internal consistency check; the values land in the range expected for 500 mg oral metformin in healthy young adults (literature Cmax ~1.0-1.8 ug/mL at Tmax 2-3 h, t1/2 ~1.5-3 h).
sim_nca <- sim |>
dplyr::filter(!is.na(Cc)) |>
dplyr::select(id, time, Cc, treatment)
# Guarantee a time=0 row per (id, treatment); pre-dose Cc = 0 for oral.
sim_nca <- dplyr::bind_rows(
sim_nca,
sim_nca |> dplyr::distinct(id, treatment) |>
dplyr::mutate(time = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, time, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, time)
dose_df <- events |>
dplyr::filter(EVID == 1L) |>
dplyr::transmute(id = ID, time = TIME, amt = AMT, treatment)
conc_obj <- PKNCA::PKNCAconc(
sim_nca, Cc ~ time | treatment + id,
concu = "ug/mL", timeu = "h"
)
dose_obj <- PKNCA::PKNCAdose(
dose_df, amt ~ time | treatment + id,
doseu = "mg"
)
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)
nca_summary <- as.data.frame(nca_res$result) |>
dplyr::group_by(PPTESTCD) |>
dplyr::summarise(
median = median(PPORRES, na.rm = TRUE),
q05 = quantile(PPORRES, 0.05, na.rm = TRUE),
q95 = quantile(PPORRES, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
dplyr::mutate(
Parameter = nlmixr2lib::ncaParamLabel(PPTESTCD)
) |>
dplyr::select(`NCA parameter` = Parameter, Median = median,
`P05` = q05, `P95` = q95)
#> Warning: There was 1 warning in `dplyr::mutate()`.
#> ℹ In argument: `Parameter = nlmixr2lib::ncaParamLabel(PPTESTCD)`.
#> Caused by warning:
#> ! ncaParamLabel(): unknown PKNCA code(s) returned as-is: 'adj.r.squared', 'clast.pred', 'lambda.z.time.first', 'lambda.z.time.last', 'r.squared', 'span.ratio'
knitr::kable(
nca_summary,
digits = 3,
caption = "Simulated NCA values from the 200-subject virtual cohort, single 500 mg PO dose. Chae 2012 does not report a paper-side NCA table for comparison.",
align = c("l", "r", "r", "r")
)| NCA parameter | Median | P05 | P95 |
|---|---|---|---|
| adj.r.squared | 0.999 | 0.999 | 1.000 |
| AUC0-∞ (obs) | 9.597 | 5.891 | 14.772 |
| Clast | 0.117 | 0.035 | 0.353 |
| clast.pred | 0.117 | 0.035 | 0.356 |
| Cmax | 1.496 | 1.088 | 2.030 |
| t½ | 2.042 | 1.721 | 3.378 |
| λz | 0.339 | 0.205 | 0.403 |
| λz n points | 3.000 | 3.000 | 3.050 |
| lambda.z.time.first | 8.000 | 7.900 | 8.000 |
| lambda.z.time.last | 12.000 | 12.000 | 12.000 |
| r.squared | 1.000 | 0.999 | 1.000 |
| span.ratio | 1.959 | 1.184 | 2.396 |
| Tlast | 12.000 | 12.000 | 12.000 |
| Tmax | 2.500 | 1.500 | 3.000 |
Assumptions and deviations
-
Paper inconsistency on IIV placement. Chae 2012
p.819 writes the final PK structural equations as
Ka = 0.41 * exp(eta1),CL/F = 52.6 * (CLcr/106.5)^0.782,V = 113 * exp(eta3)(eta2 omitted entirely from the equations, eta1 placed on Ka), but Chae 2012 Table 2 explicitly reports IIV CV% only for CL (29.7%), V (22.1%), and Hill r (4.05%) – Ka, tau, Emax, and EC50 IIV are marked “Not estimated” via the table’s dagger footnote. Table 2 carries paired bootstrap CIs for each estimated IIV. The packaged model follows Table 2 (IIV on CL, V, and Hill r) on the basis that the parameter-with-uncertainty table is the canonical source for IIV magnitude and the inline equations on p.819 contain an apparent typesetting error (eta1 likely intended for CL/F, with eta2 reserved for V and the Ka term carrying no eta). - CLcr derivation method. Chae 2012 Table 1 reports creatinine clearance in mL/min but does not state whether the values were measured directly or estimated via Cockcroft-Gault or another formula. The packaged model carries CRCL in raw mL/min (not BSA-normalised) with the reference 106.5 mL/min taken from the Chae 2012 cohort median.
-
PD endpoint scale. The structural PD output
pctEffect = M3is the percent change in plasma glucose relative to the no-metformin control arm. Chae 2012 Figure 5B shows the absolute fasting plasma glucose trajectory derived by back-conversion using each subject’s measured control-arm baseline; the packaged model emits the raw percent-effect variable so users can apply their own baseline-FPG conversion if desired. - No paper-side NCA table. Chae 2012 reports model validation through bootstrap-CI parameter precision and a visual predictive check (Figure 5) rather than a tabulated NCA comparison; the PKNCA section above therefore reports simulated NCA values only.
- Virtual cohort. The 200-subject simulation uses the published cohort demographics (age 21-31 years uniform; weight 68.63 +/- 8.14 kg Gaussian; CRCL 106.5 +/- 16 mL/min Gaussian truncated to [80, 130]; all-male healthy Korean). No baseline-FPG variability is simulated because the percent-effect endpoint cancels the baseline term out of the PD ODEs.