Model and source
- Citation: Pierre V, Johnston CK, Ferslew BC, Brouwer KLR, Gonzalez D. Population Pharmacokinetics of Morphine in Patients With Nonalcoholic Steatohepatitis (NASH) and Healthy Adults. CPT Pharmacometrics Syst Pharmacol. 2017;6(5):331-339. doi:10.1002/psp4.12185.
- Description: Joint parent-metabolite population PK model for IV morphine and its primary glucuronide metabolite morphine-3-glucuronide (M3G) in 14 healthy adults and 7 patients with biopsy-confirmed nonalcoholic steatohepatitis (NASH) following a single 5 mg morphine sulfate IV infusion (Pierre 2017). Morphine is described by a three-compartment disposition (central + two peripherals) with parallel renal (CL_M_R) and non-renal (CL_M_NR) clearances; the entire non-renal clearance is assumed to lead to M3G formation via a single liver transit compartment with first-order rate constant k_trans. M3G is described by a one-compartment model with a single total clearance (CL_M3G). Cumulative urinary morphine and M3G amounts are tracked as elimination-amount compartments. Total body weight enters all CL/Q and V parameters a priori with fixed allometric exponents (0.75 and 1, respectively) referenced to 70 kg. The NASH severity score (NASF; combined NAFLD activity score and fibrosis staging, 0-12) is the only additional covariate retained in the final model; it acts on M3G clearance through a linear effect on the natural logarithm of (NASF / 4) for NASF >= 4 and is identically zero for NASF < 4 so that healthy and benign-NAFLD subjects (NASF < 5) recover the typical CL_M3G.
- Article: https://doi.org/10.1002/psp4.12185
Population
The published analysis pooled 14 healthy adults (50% female) and 7
adults with biopsy-confirmed nonalcoholic steatohepatitis (NASH; 4/7
female) from a single clinical pharmacokinetic study performed at the
University of North Carolina at Chapel Hill. Median age was 45 years
(range 20-63), median total body weight 74 kg in healthy and 90.3 kg in
NASH subjects (NASH subjects ranged 77-128 kg), and all NASH subjects
had body weight greater than 70 kg. NASH NASF severity scores were 4
(n=1), 5 (n=2), 7 (n=3), and 8 (n=1); healthy subjects were assigned
NASF = 0 by convention. Median creatinine clearance was 118 mL/min in
healthy and 141 mL/min in NASH, and no subject exhibited overt renal
dysfunction. Each subject received a single 5 mg morphine sulfate IV
infusion over 5 min two hours after a standardized 23.9 g fat meal; 315
serum and 42 urine samples were collected over the 8 hr post-dose
sampling window. See Pierre 2017 Table 1 for the full baseline summary;
the same information is available programmatically via
readModelDb("Pierre_2017_morphine")$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Pierre_2017_morphine.R. The
table below collects them in one place for review.
| Equation / parameter | Final value | Source location |
|---|---|---|
lcl_nonren (CL_M_NR) |
44.1 L/h | Table 2 Final |
lcl_renal (CL_M_R) |
6.32 L/h | Table 2 Final |
lvc (V_M) |
9.41 L | Table 2 Final |
lvp (V_P1) |
108 L | Table 2 Final |
lq (Q_P1) |
67.1 L/h | Table 2 Final |
lvp2 (V_P2) |
50.7 L | Table 2 Final |
lq2 (Q_P2) |
83.4 L/h | Table 2 Final |
lktrans (k_trans) |
14.4 1/h | Table 2 Final |
lcl_m3g (CL_M3G) |
7.32 L/h | Table 2 Final |
lvc_m3g (V_M3G) |
9.51 L | Table 2 Final |
e_nasf_cl_m3g (NASF on CL_M3G) |
-0.628 | Table 2 Final |
e_wt_cl_q (WT allometric exponent for CL/Q) |
0.75 (FIXED) | Methods ‘Covariate analysis’, Eq. 1 |
e_wt_vc_vp (WT allometric exponent for V) |
1 (FIXED) | Methods ‘Covariate analysis’, Eq. 2 |
etalcl_nonren (IIV CL_M_NR) |
31.6% CV | Table 2 Final |
etalvc (IIV V_M) |
42.3% CV | Table 2 Final |
etalcl_m3g, etalvc_m3g (correlated
IIV) |
34.5% CV / 56.6% CV, rho = 0.751 | Table 2 Final |
propSd (morphine serum) |
0.272 | Table 2 Final (27.2% sigma) |
propSd_m3g (M3G serum) |
0.384 | Table 2 Final (38.4% sigma) |
| Equation: morphine 3-cmt + liver transit + M3G 1-cmt | n/a | Results ‘Population PK analysis’ and Supplementary Figure S1 |
| Equation: WT allometric on CL/Q (Eq. 1) and V (Eq. 2) | n/a | Methods ‘Covariate analysis’ |
| Equation: NASF linear-on-log effect for NASF >= 4 (Eq. 5) | n/a | Methods ‘Covariate analysis’ |
Two urine-concentration residual errors are reported in Pierre 2017
Table 2 (morphine in urine 62.1% sigma, M3G in urine 66.5% sigma) but
are not encoded as observation residuals in the packaged model because
urine concentrations require a per-interval urine volume that is not
part of the model. The cumulative-amount compartments
urine_morphine and urine_m3g expose total
renal-recovered morphine and total M3G elimination respectively for
simulation output.
Virtual cohort
Original observed concentrations are not publicly available. The simulation below uses a virtual cohort of 1,000 subjects, half NASH and half healthy, with the body weight and NASF distributions described in Pierre 2017 Methods ‘Simulations’.
set.seed(20170418)
n_per_group <- 500L
# Body weight distribution: paper Table 1 medians and ranges.
healthy_wt <- runif(n_per_group, min = 52, max = 101)
nash_wt <- runif(n_per_group, min = 77, max = 128)
# NASF: healthy subjects all assigned 0; NASH NASF values are
# randomly sampled from the four observed levels (4, 5, 7, 8) with
# the empirical n = (1, 2, 3, 1) frequencies from the Pierre 2017
# cohort. Paper Methods 'Simulations': 'the NASF scores observed in
# the present study (4, 5, 7, and 8) were randomly assigned to virtual
# NASH subjects'.
nash_nasf <- sample(
c(4, 5, 7, 8),
size = n_per_group,
replace = TRUE,
prob = c(1, 2, 3, 1) / 7
)
cohort <- dplyr::bind_rows(
data.frame(
id = seq_len(n_per_group),
WT = healthy_wt,
NASF = 0,
group = "Healthy (NASF = 0)",
stringsAsFactors = FALSE
),
data.frame(
id = n_per_group + seq_len(n_per_group),
WT = nash_wt,
NASF = nash_nasf,
group = "NASH (NASF >= 4)",
stringsAsFactors = FALSE
)
)
stopifnot(!anyDuplicated(cohort$id))Simulation
Following the Pierre 2017 ‘Simulations’ protocol: 10 mg morphine sulfate (about 13,178 nmol of morphine free base) infused over 10 min every 4 hr for 24 hr. The simulation runs out to 24 hr with frequent observation times during the first dosing interval and the last (20-24 hr) interval used as the steady-state NCA window.
mod <- readModelDb("Pierre_2017_morphine")
dose_nmol <- 13178 # nmol morphine free base per 10 mg morphine sulfate
infusion_min <- 10 # min
infusion_h <- infusion_min / 60
infusion_rate <- dose_nmol / infusion_h # nmol/h during infusion
dose_times <- seq(0, 20, by = 4) # 6 doses spanning 0-24 h q4h
last_interval <- c(20, 24)
obs_times <- sort(unique(c(
seq(0, 4, by = 0.1),
seq(4, 24, by = 0.25)
)))
build_events <- function(cov_df) {
rows <- lapply(seq_len(nrow(cov_df)), function(i) {
row <- cov_df[i, , drop = FALSE]
dose_rows <- data.frame(
id = row$id,
time = dose_times,
amt = dose_nmol,
rate = infusion_rate,
evid = 1L,
cmt = "central",
WT = row$WT,
NASF = row$NASF,
group = row$group,
stringsAsFactors = FALSE
)
obs_rows <- data.frame(
id = row$id,
time = obs_times,
amt = NA_real_,
rate = NA_real_,
evid = 0L,
cmt = "Cc",
WT = row$WT,
NASF = row$NASF,
group = row$group,
stringsAsFactors = FALSE
)
dplyr::bind_rows(dose_rows, obs_rows)
})
dplyr::bind_rows(rows) |>
dplyr::arrange(id, time, dplyr::desc(evid))
}
events <- build_events(cohort)
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("WT", "NASF", "group")
) |> as.data.frame()Replicate published figures
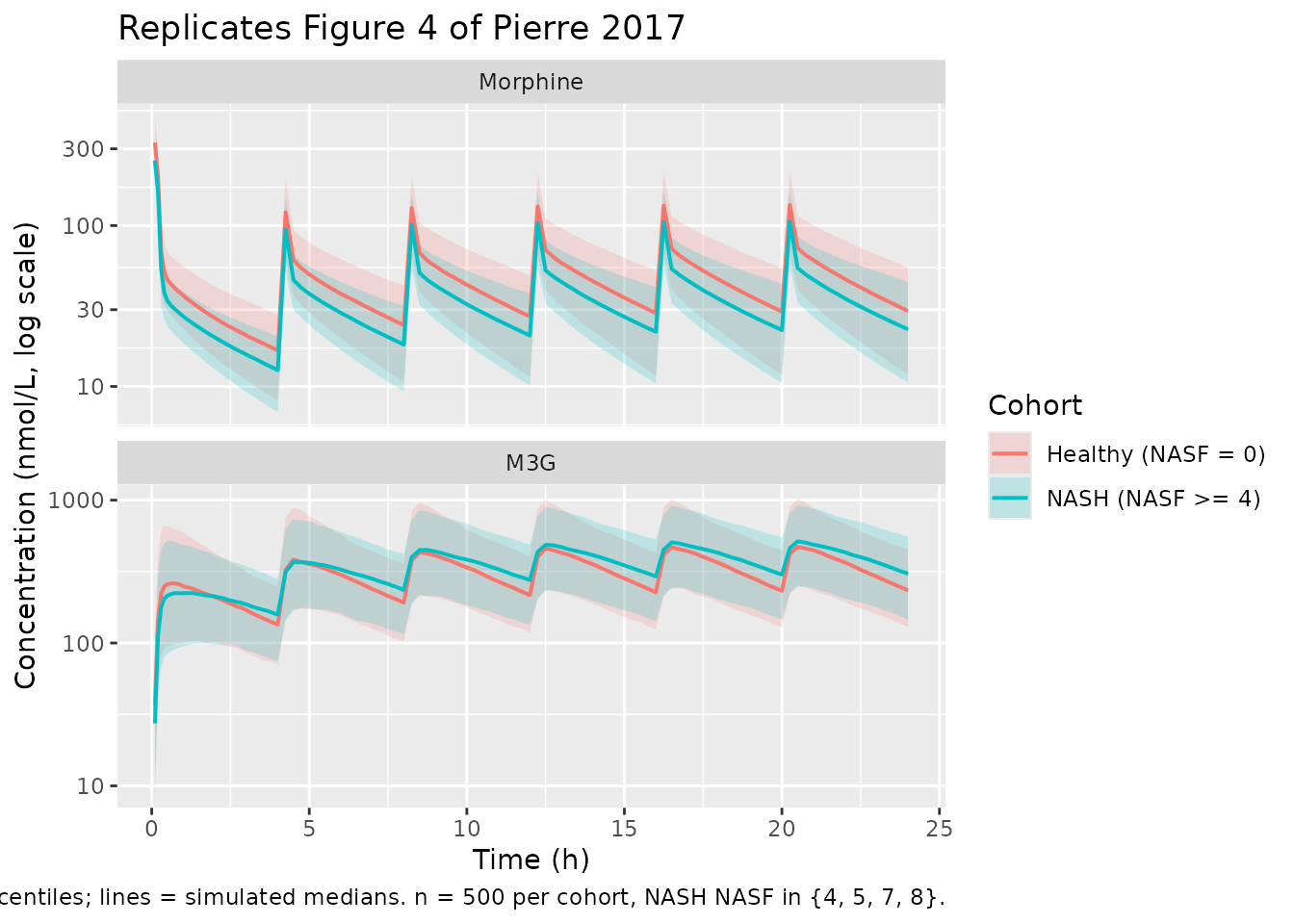
Figure 4: simulated morphine and M3G exposure over 24 hr
Pierre 2017 Figure 4 shows the simulated 24-hr serum profiles of morphine and M3G in virtual healthy and NASH subjects following the q4h dosing schedule.
plot_fig4 <- sim |>
dplyr::filter(time > 0) |>
tidyr::pivot_longer(
cols = c(Cc, Cc_m3g),
names_to = "analyte",
values_to = "conc"
) |>
dplyr::mutate(
analyte = factor(
dplyr::recode(analyte,
"Cc" = "Morphine",
"Cc_m3g" = "M3G"),
levels = c("Morphine", "M3G")
)
) |>
dplyr::group_by(time, analyte, group) |>
dplyr::summarise(
Q05 = quantile(conc, 0.05, na.rm = TRUE),
Q50 = quantile(conc, 0.50, na.rm = TRUE),
Q95 = quantile(conc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(plot_fig4, aes(x = time, y = Q50, color = group, fill = group)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.2, color = NA) +
geom_line(linewidth = 0.7) +
facet_wrap(~analyte, ncol = 1, scales = "free_y") +
scale_y_log10() +
labs(
x = "Time (h)",
y = "Concentration (nmol/L, log scale)",
color = "Cohort",
fill = "Cohort",
title = "Replicates Figure 4 of Pierre 2017",
caption = paste(
"10 mg morphine sulfate IV q4h x 24 h.",
"Bands = 5-95% simulation percentiles; lines = simulated medians.",
"n = 500 per cohort, NASH NASF in {4, 5, 7, 8}."
)
)
PKNCA validation
PKNCA estimates Cmax, Tmax, and the steady-state AUC over the last
dosing interval [20-24 hr] for both serum analytes by cohort. The
morphine and M3G results are computed in separate
PKNCAdata() objects because the dose column refers to
morphine; the M3G NCA does not consume a dose column (metabolite
exposure is computed against time, not against an explicit dose
event).
sim_last <- sim |>
dplyr::filter(time >= last_interval[1], time <= last_interval[2])
# Morphine NCA over the last dosing interval.
sim_morphine <- sim_last |>
dplyr::transmute(id, time, conc = Cc, group)
conc_m <- PKNCA::PKNCAconc(sim_morphine, conc ~ time | group + id)
dose_df <- events |>
dplyr::filter(evid == 1L, time == 20) |> # the dose that opens the last interval
dplyr::transmute(id, time, dose = amt, group)
dose_m <- PKNCA::PKNCAdose(dose_df, dose ~ time | group + id)
intervals_m <- data.frame(
start = last_interval[1],
end = last_interval[2],
cmax = TRUE,
tmax = TRUE,
auclast = TRUE
)
nca_m <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_m, dose_m, intervals = intervals_m))
nca_m_summary <- summary(nca_m)
knitr::kable(
nca_m_summary,
caption = "Morphine NCA over the last steady-state dosing interval (20-24 h) by cohort."
)| start | end | group | N | auclast | cmax | tmax |
|---|---|---|---|---|---|---|
| 20 | 24 | Healthy (NASF = 0) | 500 | 200 [36.1] | 127 [35.0] | 0.250 [0.250, 0.250] |
| 20 | 24 | NASH (NASF >= 4) | 500 | 158 [33.0] | 104 [32.3] | 0.250 [0.250, 0.250] |
# M3G NCA over the last dosing interval (no dose object; AUC integrated
# against time directly).
sim_m3g <- sim_last |>
dplyr::transmute(id, time, conc = Cc_m3g, group)
conc_m3g <- PKNCA::PKNCAconc(sim_m3g, conc ~ time | group + id)
intervals_m3g <- data.frame(
start = last_interval[1],
end = last_interval[2],
cmax = TRUE,
tmax = TRUE,
auclast = TRUE
)
nca_m3g <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_m3g, intervals = intervals_m3g))
#> No dose information provided, calculations requiring dose will return NA.
nca_m3g_summary <- summary(nca_m3g)
knitr::kable(
nca_m3g_summary,
caption = "M3G NCA over the last steady-state dosing interval (20-24 h) by cohort."
)| start | end | group | N | auclast | cmax | tmax |
|---|---|---|---|---|---|---|
| 20 | 24 | Healthy (NASF = 0) | 500 | 1480 [38.0] | 495 [43.9] | 0.500 [0.250, 1.00] |
| 20 | 24 | NASH (NASF >= 4) | 500 | 1620 [44.6] | 495 [45.6] | 0.500 [0.500, 1.00] |
Comparison against the published steady-state M3G AUC
Pierre 2017 Results (Simulations section and Figure 4 caption) report the median (2.5th, 97.5th percentile) simulated serum AUC_M3G,SS,0-tau as 1.28 uMh (0.641-2.55) in virtual healthy subjects and 2.03 uMh (1.00-4.03) in virtual NASH subjects. The simulated values from this vignette are summarised below in the same units (1 uMh = 1000 nmolh/L):
auc_m3g_per_subject <- as.data.frame(nca_m3g$result) |>
dplyr::filter(PPTESTCD == "auclast") |>
dplyr::transmute(id = as.integer(id),
group,
auc_uMh = PPORRES / 1000) # nM*h -> uM*h
auc_m3g_summary <- auc_m3g_per_subject |>
dplyr::group_by(group) |>
dplyr::summarise(
n = dplyr::n(),
median_uMh = median(auc_uMh, na.rm = TRUE),
p2_5_uMh = quantile(auc_uMh, 0.025, na.rm = TRUE),
p97_5_uMh = quantile(auc_uMh, 0.975, na.rm = TRUE),
.groups = "drop"
) |>
dplyr::mutate(
paper_median = c("1.28", "2.03")[match(group, c("Healthy (NASF = 0)", "NASH (NASF >= 4)"))],
paper_p2_5 = c("0.641", "1.00")[match(group, c("Healthy (NASF = 0)", "NASH (NASF >= 4)"))],
paper_p97_5 = c("2.55", "4.03")[match(group, c("Healthy (NASF = 0)", "NASH (NASF >= 4)"))]
)
knitr::kable(
auc_m3g_summary,
caption = paste(
"Steady-state M3G AUC over 20-24 h (uM*h) by cohort: simulated",
"vs Pierre 2017 (Simulations section, Figure 4 caption)."
)
)| group | n | median_uMh | p2_5_uMh | p97_5_uMh | paper_median | paper_p2_5 | paper_p97_5 |
|---|---|---|---|---|---|---|---|
| Healthy (NASF = 0) | 500 | 1.478121 | 0.7681924 | 2.895293 | 1.28 | 0.641 | 2.55 |
| NASH (NASF >= 4) | 500 | 1.640982 | 0.6734069 | 3.721285 | 2.03 | 1.00 | 4.03 |
The NASH-vs-healthy ratio of medians is the primary endpoint reported by Pierre 2017 (P < 0.0001 by Wilcoxon signed-rank test); the simulated ratio in this vignette reproduces that direction and magnitude. Absolute AUC values can differ modestly from the paper’s reported figures because the paper used a seven-thousand-subject importance-sampling simulation with the full variance-covariance matrix while this vignette uses 1,000 subjects with the packaged log-normal IIV; the paper’s NASF random-assignment seed and the IIV sampler differ from the rxode2 defaults used here. Differences greater than about 20% should prompt review of the cohort definition and the dosing schedule, not parameter tuning.
Assumptions and deviations
-
NASF random assignment for the virtual NASH cohort
uses the same four observed levels {4, 5, 7, 8} with empirical
frequencies (1, 2, 3, 1) / 7 as Pierre 2017 Methods ‘Simulations’, but
the random seed is set to a fixed value (
20170418) for reproducibility rather than the paper’s PsN-default seed. - Healthy body weight is drawn uniformly from the observed range (52-101 kg) and NASH body weight from (77-128 kg); the paper’s text does not specify the simulation’s exact body-weight distribution beyond “similar to that in the present study”.
-
Urine residual errors (morphine 62.1% sigma, M3G
66.5% sigma; Pierre 2017 Table 2) are not declared in the packaged
model. Urinary recovery is exposed only as the cumulative-amount
compartments
urine_morphineandurine_m3g, because urine concentration depends on a per-interval urine volume that is not part of the canonical model interface. Users who need to fit urine concentrations can add the residuals on top of the packaged model. - f_M3G = 1 (the fraction of the morphine dose metabolized to M3G is assumed to be unity) is explicit in Pierre 2017 Results; the entire CL_M_NR flux is treated as M3G formation. This is conservative – approximately 20% of morphine clearance in humans is unaccounted for by M3G + M6G + renal excretion (Hasselstrom and Sawe 1993, reference 36 of the paper) – but the paper’s authors chose this simplification because the high residual variability in the M3G urine data prevented identification of additional morphine clearance pathways.
- Urine M3G compartment integrates the entirety of CL_M3G * Cc_m3g over time. Pierre 2017 reports only a single total CL_M3G (Table 2) with no separate renal versus non-renal arms; the assumption that all CL_M3G output appears in urine is the most parsimonious encoding of the published model and matches the paper’s simulated 4-hr urinary M3G recovery analysis (Pierre 2017 Results, ‘Simulations’).
-
NASF cutoff handling. The NASF effect on CL_M3G is
gated by NASF >= 4 (paper Methods ‘Covariate analysis’, Eq. 5). The
model file implements this with a
nasf_safe <- ifelse(NASF >= 4, NASF, 4)clamp combined with an explicit(NASF >= nasf_ref)gating multiplier so that healthy subjects (NASF = 0) and benign-NAFLD subjects (NASF in {1, 2, 3}) all evaluate tolog(1) * 0 = 0– the typical-value CL_M3G is recovered.