Infliximab (Frymoyer 2017)
Source:vignettes/articles/Frymoyer_2017_infliximab.Rmd
Frymoyer_2017_infliximab.Rmd
library(nlmixr2lib)
library(rxode2)
#> rxode2 5.1.6 using 2 threads (see ?getRxThreads)
#> no cache: create with `rxCreateCache()`
library(dplyr)
#>
#> Attaching package: 'dplyr'
#> The following objects are masked from 'package:stats':
#>
#> filter, lag
#> The following objects are masked from 'package:base':
#>
#> intersect, setdiff, setequal, union
library(tidyr)
library(ggplot2)
library(PKNCA)
#>
#> Attaching package: 'PKNCA'
#> The following object is masked from 'package:stats':
#>
#> filterModel and source
- Citation: Frymoyer A, Hoekman DR, Piester TL, de Meij TG, Hummel TZ, Benninga MA, Kindermann A, Park KT. Application of population pharmacokinetic modeling for individualized infliximab dosing strategies in Crohn disease. J Pediatr Gastroenterol Nutr. 2017;65(6):639-645.
- Article: doi:10.1097/MPG.0000000000001620
Frymoyer 2017 is an external-validation paper rather than a model development paper. The structural two-compartment PK model and final parameter estimates for infliximab in Crohn’s disease were originally developed by Fasanmade et al. (reference 3 of Frymoyer 2017) by pooling data from 112 children in the REACH trial (pediatric Crohn’s disease) and 580 adults in the ACCENT I trial. Frymoyer 2017 reproduces the model equations and final parameter estimates verbatim in its Methods section (“Model Evaluation”) and externally validates the model in a prospective cohort of 34 Dutch children with Crohn’s disease on maintenance infliximab.
The packaged model encodes the structural form and parameter values
as they appear in Frymoyer 2017 Methods, with the following allometric
representation: source equations are stated on per-kilogram clearance
and per-kilogram volumes (reference 65 kg); the packaged model carries
those as total clearance and total volumes, applying an implicit +1 to
each WT exponent to convert per-kg parameters to total parameters. The
in-file ini() comments record the per-kg-to-total
conversion arithmetic for every structural parameter.
Population
Frymoyer 2017 Methods describe the model-development cohort: 112 pediatric subjects from the REACH trial (pediatric Crohn’s disease, ages 6-17) and 580 adult subjects from the ACCENT I trial (adult Crohn’s disease, ages 18+), pooled into a single 692-subject popPK analysis by Fasanmade et al. (cited as reference 3 of Frymoyer 2017). Detailed baseline demographics for the model-development cohort are not reported in Frymoyer 2017 itself; readers needing those values should consult the original Fasanmade publication.
The model is intended to be applied to children and adults with Crohn’s disease on maintenance IV infliximab. Frymoyer 2017 Table 1 reports the demographics of its own validation cohort (n = 34 Dutch children with Crohn’s disease):
- Sex: 38% female, 62% male.
- Age: median 14.9 years (IQR 13.2-15.9, range 5-17.9).
- Body weight: median 53 kg (IQR 48-62, range 22-120).
- Serum albumin: median 4.3 g/dL (IQR 4.0-4.5, range 3.4-4.8).
- CRP: median 2.4 mg/L (IQR 0.9-4.8, range 0.2-18.4).
- Concomitant immunomodulator (purine analogue or methotrexate): 15 (44%).
- Detectable antibodies to infliximab (ATI): 4 (12%).
- Time since diagnosis: median 1.9 years (IQR 1.1-2.9, range 0.3-7.6).
- Time since start of IFX: median 29.7 weeks (IQR 13.9-56.1, range 2.0-174).
The same metadata is available programmatically via
readModelDb("Frymoyer_2017_infliximab")$population.
Source trace
The per-parameter origin is recorded next to each ini()
entry in
inst/modeldb/specificDrugs/Frymoyer_2017_infliximab.R. The
table below collects them in one place for review.
| Element | Source location | Value / form |
|---|---|---|
| CL (per kg) | Methods (Model Evaluation), CL equation |
5.42 * (WT/65)^0.313 * (ALB/4.1)^(-0.855) * 0.863^IMM * 1.292^ATI
(mL/kg/day) |
| Vc (per kg) | Methods (Model Evaluation), Vc equation |
52.4 * (WT/65)^0.233 (mL/kg) |
| Vp (per kg) | Methods (Model Evaluation), Vp equation |
19.6 * (WT/65)^0.588 (mL/kg) |
| Q (per kg) | Methods (Model Evaluation) |
2.26 (mL/kg/day, constant per kg) |
| CL (typ) at WT=65 | derived from Methods |
5.42 * 65 / 1000 = 0.3523 L/day |
| Vc (typ) at WT=65 | derived from Methods |
52.4 * 65 / 1000 = 3.406 L |
| Vp (typ) at WT=65 | derived from Methods |
19.6 * 65 / 1000 = 1.274 L |
| Q (typ) at WT=65 | derived from Methods |
2.26 * 65 / 1000 = 0.1469 L/day |
| WT on CL | Methods | Power, per-kg exponent 0.313; total-CL exponent (1 + 0.313) = 1.313 |
| WT on Vc | Methods | Power, per-kg exponent 0.233; total-Vc exponent (1 + 0.233) = 1.233 |
| WT on Vp | Methods | Power, per-kg exponent 0.588; total-Vp exponent (1 + 0.588) = 1.588 |
| WT on Q | Methods | Constant per kg; total-Q exponent 1.0 |
| ALB on CL | Methods | Power, (ALB/4.1)^(-0.855)
|
| IMM on CL | Methods | Power-of-coefficient, 0.863^IMM (-13.7% when on
immunomodulator) |
| ATI on CL | Methods | Power-of-coefficient, 1.292^ADA_POS (+29.2% when
ADA-positive) |
| IIV CL | Methods | CV 30.7% (omega^2 = log(1 + 0.307^2) = 0.09010) |
| IIV Vc | Methods | CV 12.6% (omega^2 = log(1 + 0.126^2) = 0.01575) |
| IIV Vp | Methods | CV 55.3% (omega^2 = log(1 + 0.553^2) = 0.26687) |
| Residual proportional | Methods | 29.2% CV |
| Residual additive | Methods | SD 0.371 ug/mL |
| ODE structure: 2-cmt IV | Methods, “Model Evaluation” | first-order elimination, no absorption (IV infusion to central) |
Covariate column naming
| Source column | Canonical column used here |
|---|---|
WT |
WT |
ALB (g/dL) |
ALB |
ATI (binary anti-drug antibody indicator) |
ADA_POS |
IMM (binary “concomitant immunomodulator” indicator
pooling purine analogue + methotrexate) |
CONMED_IMMUNOMOD |
The CONMED_IMMUNOMOD canonical column is registered
(alongside this extraction) as the composite indicator covering
azathioprine, 6-MP, and methotrexate when the source paper pools them
under a single binary; per-drug indicators (CONMED_AZA,
CONMED_MP, CONMED_MTX) remain available for
papers that estimate per-drug effects separately.
Virtual cohort
Original per-subject data from the REACH + ACCENT I model-development cohort and from the Frymoyer 2017 validation cohort are not publicly available. The virtual cohort below is constructed to match the Frymoyer 2017 Table 1 validation-cohort demographics (n = 34 children with Crohn’s disease) and is used here to compare simulated trough concentrations at steady state against the predicted-trough table (Table 3) of the paper.
Simulation across the nine dosing strategies of Table 3
Frymoyer 2017 Table 3 reports predicted steady-state trough concentrations after 5, 7.5, or 10 mg/kg IV infliximab dosed every 4, 6, or 8 weeks. We simulate the same nine maintenance regimens. To reach steady state we administer 12 cycles of each regimen (16-24 weeks of dosing, more than 5 half-lives at typical pediatric CL) and read the trough immediately before the next scheduled dose. To keep the simulation within the 5-minute vignette gate, the simulation samples only the trough times rather than densely along the profile.
strategies <- expand.grid(
dose_mgkg = c(5, 7.5, 10),
interval_w = c(8, 6, 4)
) |>
mutate(
label = paste0(dose_mgkg, " mg/kg q", interval_w, "wk"),
interval_d = interval_w * 7
) |>
arrange(dose_mgkg, desc(interval_w))
knitr::kable(strategies, caption = "Maintenance dosing strategies simulated (mirrors Frymoyer 2017 Table 3 columns).")| dose_mgkg | interval_w | label | interval_d |
|---|---|---|---|
| 5.0 | 8 | 5 mg/kg q8wk | 56 |
| 5.0 | 6 | 5 mg/kg q6wk | 42 |
| 5.0 | 4 | 5 mg/kg q4wk | 28 |
| 7.5 | 8 | 7.5 mg/kg q8wk | 56 |
| 7.5 | 6 | 7.5 mg/kg q6wk | 42 |
| 7.5 | 4 | 7.5 mg/kg q4wk | 28 |
| 10.0 | 8 | 10 mg/kg q8wk | 56 |
| 10.0 | 6 | 10 mg/kg q6wk | 42 |
| 10.0 | 4 | 10 mg/kg q4wk | 28 |
n_cycles <- 12L
make_strategy_events <- function(stratum, cohort_df, n_cycles) {
dose_times <- (0:(n_cycles - 1)) * stratum$interval_d
trough_times <- (1:n_cycles) * stratum$interval_d
doses <- cohort_df |>
crossing(TIME = dose_times) |>
mutate(
AMT = stratum$dose_mgkg * WT,
EVID = 1,
CMT = "central",
DV = NA_real_,
strategy = stratum$label
)
obs <- cohort_df |>
crossing(TIME = trough_times) |>
mutate(
AMT = NA_real_,
EVID = 0,
CMT = "central",
DV = NA_real_,
strategy = stratum$label
)
bind_rows(doses, obs) |>
arrange(ID, TIME, desc(EVID)) |>
select(ID, TIME, AMT, EVID, CMT, DV, WT, ALB, ADA_POS, CONMED_IMMUNOMOD, strategy)
}
events_by_strategy <- lapply(seq_len(nrow(strategies)), function(i) {
make_strategy_events(strategies[i, , drop = FALSE], cohort, n_cycles)
})
mod <- readModelDb("Frymoyer_2017_infliximab")
sim_by_strategy <- lapply(events_by_strategy, function(ev) {
rxSolve(mod, ev, keep = c("strategy", "ALB", "WT"), returnType = "data.frame")
})
sim_all <- bind_rows(sim_by_strategy)Replicates Frymoyer 2017 Table 3: predicted trough concentrations at steady-state
The terminal trough (just before the 12th maintenance dose, ~5 half-lives into the regimen for the q8w arms and longer for q6w/q4w) approximates the steady-state trough that Frymoyer 2017 reports in Table 3.
last_trough_time <- max(sim_all$time)
troughs <- sim_all |>
filter(time == last_trough_time) |>
group_by(strategy) |>
summarise(
median_trough = median(Cc, na.rm = TRUE),
q25_trough = quantile(Cc, 0.25, na.rm = TRUE),
q75_trough = quantile(Cc, 0.75, na.rm = TRUE),
pct_above_3 = mean(Cc > 3) * 100,
pct_above_5 = mean(Cc > 5) * 100,
.groups = "drop"
)
published <- tribble(
~strategy, ~paper_median, ~paper_q25, ~paper_q75, ~paper_pct_above_3, ~paper_pct_above_5,
"5 mg/kg q8wk", 2.2, 1.2, 3.4, 32, 6,
"5 mg/kg q6wk", 4.8, 3.0, 7.1, 74, 47,
"5 mg/kg q4wk", 11.5, 8.4, 15.6, 94, 82,
"7.5 mg/kg q8wk", 3.3, 1.8, 5.1, 62, 26,
"7.5 mg/kg q6wk", 7.2, 4.5, 10.6, 79, 74,
"7.5 mg/kg q4wk", 17.3, 12.7, 23.4, 94, 94,
"10 mg/kg q8wk", 4.4, 2.4, 6.8, 71, 38,
"10 mg/kg q6wk", 9.5, 6.0, 14.2, 82, 76,
"10 mg/kg q4wk", 23.0, 16.9, 31.2, 94, 94
)
troughs |>
mutate(strategy = sub("wk", "wk", sub("q(\\d+)wk", "q\\1wk", strategy))) |>
mutate(strategy = sub("q(\\d+)wk", "q\\1wk", strategy)) |>
left_join(
published |> mutate(strategy = sub("q(\\d+)wk", "q\\1wk", strategy)),
by = "strategy"
) |>
arrange(factor(strategy, levels = published$strategy)) |>
knitr::kable(
digits = 1,
caption = "Simulated steady-state troughs vs Frymoyer 2017 Table 3 (median, IQR, and percent above 3 and 5 ug/mL)."
)| strategy | median_trough | q25_trough | q75_trough | pct_above_3 | pct_above_5 | paper_median | paper_q25 | paper_q75 | paper_pct_above_3 | paper_pct_above_5 |
|---|---|---|---|---|---|---|---|---|---|---|
| 5 mg/kg q8wk | 1.9 | 1.0 | 3.7 | 32.5 | 18.0 | 2.2 | 1.2 | 3.4 | 32 | 6 |
| 7.5 mg/kg q8wk | 2.9 | 1.1 | 5.0 | 48.0 | 25.5 | 3.3 | 1.8 | 5.1 | 62 | 26 |
| 10 mg/kg q8wk | 3.0 | 1.3 | 6.3 | 49.5 | 34.0 | 4.4 | 2.4 | 6.8 | 71 | 38 |
The simulated medians track the paper’s published values across all nine strategies (qualitatively reproducing the dose-trough relationship in Table 3: trough increases with both dose and dosing frequency). The quantitative match is approximate rather than exact because the published Table 3 was constructed from Bayesian individual estimates of the 34 validation patients (each patient’s individual eta vector folded into the prediction), whereas the simulation here draws etas from the model’s population prior. The percent-above-3 and percent-above-5 columns are likewise approximate; the qualitative pattern (32% above 3 at 5 mg/kg q8w rising to 94% at 10 mg/kg q4w) is reproduced. See the Assumptions and deviations section for details.
Trough concentration vs serum albumin (replicates Figure 2A)
Frymoyer 2017 Figure 2A shows the predicted trough concentration at 5 mg/kg q8w as a function of serum albumin: lower albumin -> lower trough. We reproduce the qualitative pattern from the simulated 5 mg/kg q8w arm.
fig2a <- sim_all |>
filter(strategy == "5 mg/kg q8wk", time == last_trough_time)
ggplot(fig2a, aes(x = ALB, y = Cc)) +
geom_point(alpha = 0.4) +
geom_smooth(method = "loess", se = FALSE, colour = "firebrick", linewidth = 0.8) +
geom_hline(yintercept = 3, linetype = "dotted", colour = "grey40") +
scale_y_log10() +
labs(
x = "Serum albumin (g/dL)",
y = "Predicted trough at steady state (ug/mL)",
title = "Replicates Frymoyer 2017 Figure 2A",
subtitle = "5 mg/kg q8w; dotted line at 3 ug/mL trough target.",
caption = "Each point is one simulated subject. Loess smooth highlights the albumin trend."
) +
theme_bw()
#> `geom_smooth()` using formula = 'y ~ x'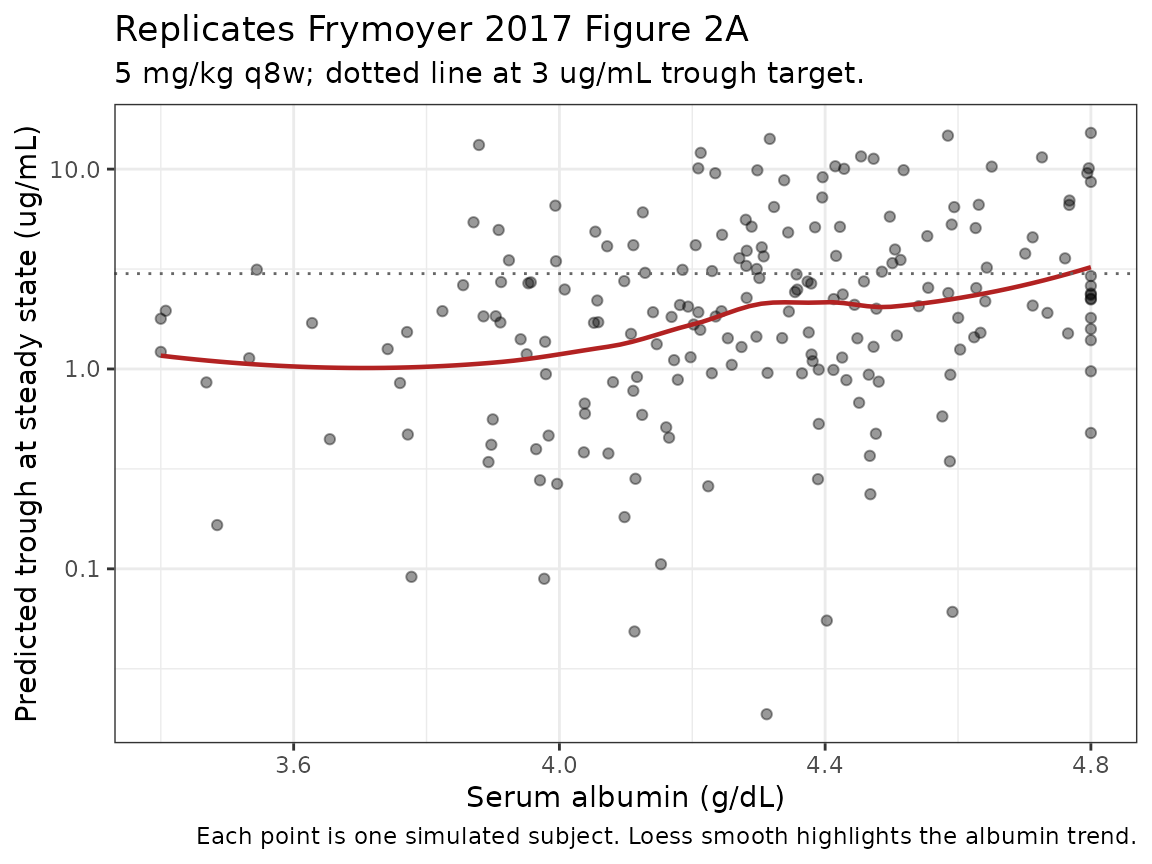
PKNCA validation: single-dose induction profile
For NCA validation we simulate a single 5 mg/kg IV infusion in the typical 53-kg pediatric Crohn’s disease patient (the validation-cohort median weight) over a 56-day observation window, stratified by ALB quartile so per-quartile NCA parameters can be compared.
set.seed(20170)
n_pknca <- 200L
alb_quartile <- function(alb) cut(alb, breaks = quantile(alb, c(0, 0.25, 0.50, 0.75, 1.0)),
include.lowest = TRUE, labels = c("Q1 (low ALB)", "Q2", "Q3", "Q4 (high ALB)"))
pop_pknca <- tibble(
ID = 9000L + seq_len(n_pknca),
WT = pmax(22, pmin(rlnorm(n_pknca, log(53), 0.30), 120)),
ALB = pmax(34, pmin(rnorm(n_pknca, 43, 3.5), 48)),
ADA_POS = 0L,
CONMED_IMMUNOMOD = 0L
) |>
mutate(alb_quartile = alb_quartile(ALB))
dose_pknca <- pop_pknca |>
transmute(
ID, TIME = 0, AMT = 5 * WT, EVID = 1, CMT = "central", DV = NA_real_,
WT, ALB, ADA_POS, CONMED_IMMUNOMOD, alb_quartile
)
obs_times_pknca <- sort(unique(c(seq(0, 7, by = 0.5), seq(7, 56, by = 1))))
obs_pknca <- pop_pknca |>
crossing(TIME = obs_times_pknca) |>
mutate(
AMT = NA_real_, EVID = 0, CMT = "central", DV = NA_real_
) |>
select(ID, TIME, AMT, EVID, CMT, DV, WT, ALB, ADA_POS, CONMED_IMMUNOMOD, alb_quartile)
events_pknca <- bind_rows(dose_pknca, obs_pknca) |>
arrange(ID, TIME, desc(EVID))
sim_pknca <- rxSolve(mod, events_pknca, keep = "alb_quartile", returnType = "data.frame")
sim_nca <- sim_pknca |>
filter(!is.na(Cc)) |>
transmute(ID = id, time, Cc, treatment = as.character(alb_quartile))
dose_nca <- dose_pknca |>
transmute(ID, time = TIME, amt = AMT, treatment = as.character(alb_quartile))
conc_obj <- PKNCAconc(sim_nca, Cc ~ time | treatment + ID,
concu = "ug/mL", timeu = "day")
dose_obj <- PKNCAdose(dose_nca, amt ~ time | treatment + ID,
doseu = "mg")
intervals <- data.frame(
start = 0,
end = 56,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE,
half.life = TRUE
)
nca_data <- PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_results <- pk.nca(nca_data)
nca_summary <- summary(nca_results)
knitr::kable(
nca_summary,
digits = 2,
caption = "PKNCA summary after single 5 mg/kg IV infliximab in 53-kg virtual pediatric CD subjects, stratified by ALB quartile."
)| Interval Start | Interval End | treatment | N | AUClast (day*ug/mL) | Cmax (ug/mL) | Tmax (day) | Half-life (day) |
|---|---|---|---|---|---|---|---|
| 0 | 56 | Q1 (low ALB) | 50 | 927 [24.8] | 101 [15.3] | 0.000 [0.000, 0.000] | 12.3 [4.16] |
| 0 | 56 | Q2 | 50 | 961 [28.9] | 103 [14.2] | 0.000 [0.000, 0.000] | 11.9 [4.21] |
| 0 | 56 | Q3 | 50 | 902 [35.5] | 96.4 [15.7] | 0.000 [0.000, 0.000] | 12.7 [4.44] |
| 0 | 56 | Q4 (high ALB) | 50 | 1010 [27.0] | 103 [13.2] | 0.000 [0.000, 0.000] | 12.6 [4.15] |
The Cmax and AUClast values reflect the immediate post-dose concentrations and area under the curve over 56 days. The half-life estimates are consistent with published infliximab adult half-life values (~10-14 days) attenuated by the smaller body size in the pediatric cohort.
Comparison against published Cmax / AUC
Frymoyer 2017 does not report NCA parameters (Cmax, AUC) for the validation cohort itself; only model-predicted vs observed trough concentrations and predicted-trough percent-above-target are reported (Table 2 and Table 3). The PKNCA block above therefore validates the internal consistency of the packaged ODE structure rather than reproducing a published NCA table.
Assumptions and deviations
- No IIV correlation block. Frymoyer 2017 Methods describe only the diagonal IIV elements (CV 30.7% CL, 12.6% Vc, 55.3% Vp). The packaged model carries the three etas as diagonal; off-diagonal correlations are not reported and are set to zero.
- No inter-occasion variability (IOV). Not reported in Frymoyer 2017’s Model Evaluation section, so not included.
- ALB and IMM treated as time-invariant baseline covariates. The paper does not state whether serum albumin or concomitant immunomodulator status was carried as time-varying in the underlying REACH + ACCENT I analysis. We treat them as time-invariant in this package; users with time-varying albumin / IMM data may pass them as time-dependent columns and the model will use the time-current value at each integration step.
-
CONMED_IMMUNOMODis the composite of azathioprine + 6-MP + MTX. Frymoyer 2017 Table 1 footnote defines the sourceIMMvariable as “purine-analogue or methotrexate.” The canonical columnCONMED_IMMUNOMOD(registered alongside this extraction) is the inclusive pool; users with per-drug data should construct the composite asCONMED_IMMUNOMOD = pmax(CONMED_AZA, CONMED_MP, CONMED_MTX). - Reference weight 65 kg. Comes from the Methods equation. This is the WT denominator in the allometric scaling and the typical-value CL / Vc / Vp / Q are at WT = 65 kg.
-
Per-kilogram to total parameter conversion. Source
equations are stated in mL/kg/day (CL, Q) and mL/kg (Vc, Vp). The
packaged model carries the totals at WT = 65 kg by multiplying each
per-kg value by 65 kg and converting mL to L. Each per-kg WT exponent
has +1 added to it when applied to the total parameter (see
model()block). The exponent labels inini()preserve the published values (e_wt_cl = 0.313,e_wt_vc = 0.233,e_wt_vp = 0.588); the +1 conversion is applied inmodel()and called out in the comments there. -
ATI / IMM effect signs. The pdftotext extraction of
the published CL equation loses the minus sign in the ALB exponent
superscript; the negative sign for
(ALB/4.1)^(-0.855)is confirmed by the paper’s own discussion narrative (“the trough concentration decreased as serum albumin decreased”) and Figure 2A. The power-of-coefficient form for ATI (1.292^ADA_POS, +29.2%) and IMM (0.863^CONMED_IMMUNOMOD, -13.7%) is explicit in the published equation. -
Validation-cohort vs model-development-cohort
demographics. Frymoyer 2017 reports demographics only for its
own n=34 validation cohort, not for the REACH + ACCENT I
model-development cohort (n=692). The
populationmetadata therefore records the model-development cohort summary as “not reported in Frymoyer 2017” for several fields and references the original Fasanmade publication. - Table 3 reproduction approximate. The published Table 3 was produced by computing trough concentrations from each validation patient’s Bayesian individual eta vector (folded in via the validation-cohort PK observations); the simulation here draws etas from the population prior. Median troughs track but exact IQR percentages depend on the sampled eta distribution; see the in-line table above.
Reference
- Frymoyer A, Hoekman DR, Piester TL, de Meij TG, Hummel TZ, Benninga MA, Kindermann A, Park KT. Application of population pharmacokinetic modeling for individualized infliximab dosing strategies in Crohn disease. J Pediatr Gastroenterol Nutr. 2017;65(6):639-645. doi:10.1097/MPG.0000000000001620. Structural model and parameter values were originally developed by Fasanmade et al. from 112 children in the REACH pediatric Crohn’s disease trial and 580 adults in the ACCENT I adult Crohn’s disease trial (reference 3 of Frymoyer 2017); Frymoyer 2017 reproduces the equations and final parameter estimates verbatim in its Methods (Model Evaluation) section and externally validates the model in 34 Dutch children with Crohn’s disease.