Olodaterol (Borghardt 2016)
Source:vignettes/articles/Borghardt_2016_olodaterol.Rmd
Borghardt_2016_olodaterol.RmdModel and source
- Citation: Borghardt JM, Weber B, Staab A, Kunz C, Formella S, Kloft C. (2016). Investigating pulmonary and systemic pharmacokinetics of inhaled olodaterol in healthy volunteers using a population pharmacokinetic approach. Br J Clin Pharmacol 81(3):538-552.
- Article: https://doi.org/10.1111/bcp.12780
mod_meta <- rxode2::rxode(readModelDb("Borghardt_2016_olodaterol"))
#> ℹ parameter labels from comments will be replaced by 'label()'
mod_meta$description
#> [1] "Population PK model for inhaled and intravenous olodaterol (long-acting beta-2-adrenergic receptor agonist) in 148 healthy adult volunteers from three Phase I trials (Borghardt 2016). Four-compartment systemic disposition (central + 3 peripheral) fitted to IV plasma + urine data, with two parallel first-order elimination processes from the central compartment: renal (cl_renal) and nonrenal (cl_nonren). For inhaled administration via the Respimat inhaler, three parallel first-order absorption depots (slow, intermediate, fast) feed the central compartment, with absorption half-lives of 21.8 h, 2.00 h, and 0.268 h respectively. The pulmonary bioavailable fraction (49.4% of the nominal ex-mouthpiece dose) is split across the three depots by two logit-transformed proportionality parameters. Smoking is a covariate on the slow and fast absorption rate constants (active smokers vs ex-smokers and never-smokers pooled). Systemic disposition parameters were estimated from IV data and fixed when fitting the inhalation data."
mod_meta$reference
#> [1] "Borghardt JM, Weber B, Staab A, Kunz C, Formella S, Kloft C. Investigating pulmonary and systemic pharmacokinetics of inhaled olodaterol in healthy volunteers using a population pharmacokinetic approach. Br J Clin Pharmacol. 2016;81(3):538-552. doi:10.1111/bcp.12780."
mod_meta$units
#> $time
#> [1] "h"
#>
#> $dosing
#> [1] "ug"
#>
#> $concentration
#> [1] "pg/mL"Population
Borghardt 2016 pooled plasma and urine pharmacokinetic data from three Phase I clinical trials in 148 healthy adult volunteers (Table 1):
- Trial 1 (NCT02172131): 48 male volunteers receiving single intravenous infusions of 0.5-25 ug olodaterol over 30 min (low doses) or 3 h (high doses).
- Trial 2 (NCT02171780): 65 volunteers (9.2% female) receiving single inhaled rising doses of 2.5-70 ug olodaterol via the Respimat soft mist inhaler.
- Trial 3 (NCT02171806): 35 volunteers (25.7% female) receiving once-daily inhaled doses of 2.5, 10, or 30 ug olodaterol via Respimat for 14 days.
Pooled across trials: 133 male and 15 female volunteers
(approximately 10% female; trial 1 was 100% male). Smoking-status mix
(nonsmoker / ex-smoker / current smoker) was approximately 65 / 16 / 19%
across the pooled cohort. Body weight medians ranged 78-81 kg (range
53-105 kg); creatinine clearance medians ranged 116-121 mL/min across
the three trials. Renal function was adequate in all subjects. The same
metadata is available programmatically via
readModelDb("Borghardt_2016_olodaterol")$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Borghardt_2016_olodaterol.R. The
table below collects them in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
lvc (log VC) |
log(23.5 L) | Borghardt 2016 Table 2 (VC = 23.5 L, 4.35% RSE) |
lvp (log V2) |
log(2590 L) | Borghardt 2016 Table 2 (V2 = 2590 L, 35.7% RSE) |
lvp2 (log V3) |
log(473 L) | Borghardt 2016 Table 2 (V3 = 473 L, 10.7% RSE) |
lvp3 (log V4) |
log(16.1 L) | Borghardt 2016 Table 2 (V4 = 16.1 L, 19.7% RSE) |
lq (log Q2) |
log(31.7 L/h) | Borghardt 2016 Table 2 (Q2 = 31.7 L/h, 12.3% RSE) |
lq2 (log Q3) |
log(65.7 L/h) | Borghardt 2016 Table 2 (Q3 = 65.7 L/h, 5.28% RSE) |
lq3 (log Q4) |
log(22.5 L/h) | Borghardt 2016 Table 2 (Q4 = 22.5 L/h, 8.06% RSE) |
lcl_renal (log CL_R) |
log(10.5 L/h) | Borghardt 2016 Table 2 (CL_R = 10.5 L/h, 4.55% RSE) |
lcl_nonren (log CL_NR) |
log(63.7 L/h) | Borghardt 2016 Table 2 (CL_NR = 63.7 L/h, 8.49% RSE) |
lka_slow (log ka_slow) |
log(0.0318 1/h) | Borghardt 2016 Table 2 (ka_slow = 0.0318 1/h, 5.23% RSE) |
lka_int (log ka_int) |
log(0.347 1/h) | Borghardt 2016 Table 2 (ka_int = 0.347 1/h, 7.04% RSE) |
lka_fast (log ka_fast) |
log(2.59 1/h) | Borghardt 2016 Table 2 (ka_fast = 2.59 1/h, 9.97% RSE) |
logitpbio (logit PBIO) |
logit(0.494) = -0.024 | Borghardt 2016 Table 2 (PBIO = 49.4% of ND, 3.32% RSE) |
logitff1 (logit FF1) |
logit(0.701) = 0.852 | Borghardt 2016 Table 2 (FF1 = 70.1%, 2.33% RSE) |
logitff2 (logit FF2) |
logit(0.889) = 2.080 | Borghardt 2016 Table 2 (FF2 = 88.9%, 1.89% RSE) |
e_smoke_ka_slow |
-0.380 | Borghardt 2016 Table 2 (smoking impact on ka_slow = -0.380, 10.2% RSE) |
e_smoke_ka_fast |
1.08 | Borghardt 2016 Table 2 (smoking impact on ka_fast = 1.08, 18.0% RSE) |
etalvc, etalq, etalq2,
etalcl_nonren
|
log(1 + CV^2) for CV = 26.2 / 25.7 / 16.8 / 26.8% | Borghardt 2016 Table 2 (BSV column for VC / Q2 / Q3 / CL_NR) |
etalogitff1, etalogitff2
|
log(1 + CV^2) for CV = 11.4 / 9.33% | Borghardt 2016 Table 2 (BSV column for FF1 / FF2) |
etalogitpbio |
log(1 + 0.322^2) = 0.0987 | Borghardt 2016 Table 2 (BOV column for PBIO = 32.2% CV; encoded as BSV-equivalent here, see Assumptions and deviations) |
propSd (plasma proportional residual) |
0.158 | Borghardt 2016 Table 2 (plasma proportional RSV = 15.8% CV, 1.66% RSE) |
addSd (plasma additive residual, fixed) |
0.00001 pg/mL | Borghardt 2016 Table 2 (plasma additive RSV = 0.00001 pg/mL, fixed) |
| Three parallel-absorption depots (slow / int / fast) into central | n/a | Borghardt 2016 Figure 2 (top box) and Methods, Structural model |
| Two parallel first-order elimination routes (CL_R + CL_NR) from central | n/a | Borghardt 2016 Methods, Structural model first paragraph |
| Per-depot fractions: slow = FF1, int = (1 - FF1) * FF2, fast = (1 - FF1) * (1 - FF2) | n/a | Borghardt 2016 Methods, Structural model paragraph (proportionality parameters) |
| Dose split: f(depot) = pbio * frac_slow, f(depot2) = pbio * frac_int, f(depot3) = pbio * frac_fast | n/a | Borghardt 2016 Methods, Structural model |
| Smoker rate constants: ka_slow_smoker = ka_slow * (1 + (-0.380)), ka_fast_smoker = ka_fast * (1 + 1.08) | n/a | Borghardt 2016 Table 3 (derived smoker values) |
| Logit transformation for PBIO / FF1 / FF2 | n/a | Borghardt 2016 Methods, Random-effects model paragraph |
Virtual cohort
The cohort below mirrors the pooled trial population: 50 healthy adult volunteers, approximately 19% active smokers (matching the pooled trial-cohort smoking prevalence; ex-smokers and never-smokers are pooled to SMOKE = 0 because the paper found no PK difference between those subgroups). Two treatment arms are simulated:
- Single 10 ug intravenous infusion over 30 min (matches trial 1 intermediate dose; covers the absorption-process-independent terminal disposition curve).
- Single 10 ug oral inhalation via Respimat (matches a representative trial 2 dose); each inhaled dose enters as three simultaneous dose rows pointing at the three pulmonary depots (slow, intermediate, fast), with bioavailabilities f(depot_k) defined inside the model.
set.seed(20260618)
n_subjects <- 50L
dose_ug <- 10
obs_times <- c(0, 0.083, 0.167, 0.25, 0.33, 0.5, 0.75, 1, 1.5, 2, 3, 4,
6, 8, 10, 12, 16, 20, 24, 36, 48, 72, 96)
infusion_dur <- 0.5 # 30 min IV infusion
smoking_prob <- 0.19
# Per-subject smoking indicators (one draw per subject per arm).
smoke_iv <- stats::rbinom(n_subjects, size = 1, prob = smoking_prob)
smoke_inh <- stats::rbinom(n_subjects, size = 1, prob = smoking_prob)
make_iv_arm <- function(n, id_offset, smoke_vec) {
ids <- id_offset + seq_len(n)
smoke_lkp <- tibble(id = ids, SMOKE = as.integer(smoke_vec))
dose <- tibble(id = ids, time = 0, amt = dose_ug, cmt = "central",
evid = 1L, rate = dose_ug / infusion_dur,
treatment = "IV 10 ug")
obs <- tidyr::expand_grid(id = ids, time = obs_times) |>
dplyr::mutate(amt = 0, cmt = "central", evid = 0L, rate = 0,
treatment = "IV 10 ug")
dplyr::bind_rows(dose, obs) |>
dplyr::left_join(smoke_lkp, by = "id") |>
dplyr::arrange(id, time, dplyr::desc(evid))
}
make_inh_arm <- function(n, id_offset, smoke_vec) {
ids <- id_offset + seq_len(n)
smoke_lkp <- tibble(id = ids, SMOKE = as.integer(smoke_vec))
# One inhaled administration enters as three simultaneous dose rows
# pointing at depot / depot2 / depot3. The model's f() expressions
# split the bioavailable fraction across the three depots.
d_slow <- tibble(id = ids, time = 0, amt = dose_ug, cmt = "depot",
evid = 1L, rate = 0, treatment = "Inhaled 10 ug")
d_int <- tibble(id = ids, time = 0, amt = dose_ug, cmt = "depot2",
evid = 1L, rate = 0, treatment = "Inhaled 10 ug")
d_fast <- tibble(id = ids, time = 0, amt = dose_ug, cmt = "depot3",
evid = 1L, rate = 0, treatment = "Inhaled 10 ug")
obs <- tidyr::expand_grid(id = ids, time = obs_times) |>
dplyr::mutate(amt = 0, cmt = "central", evid = 0L, rate = 0,
treatment = "Inhaled 10 ug")
dplyr::bind_rows(d_slow, d_int, d_fast, obs) |>
dplyr::left_join(smoke_lkp, by = "id") |>
dplyr::arrange(id, time, dplyr::desc(evid))
}
events_iv <- make_iv_arm (n_subjects, id_offset = 0L, smoke_iv)
events_inh <- make_inh_arm(n_subjects, id_offset = n_subjects, smoke_inh)
events <- dplyr::bind_rows(events_iv, events_inh)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))
cat("Subjects per arm:", n_subjects,
" | IV smokers:", sum(smoke_iv),
" | Inhaled smokers:", sum(smoke_inh), "\n")
#> Subjects per arm: 50 | IV smokers: 11 | Inhaled smokers: 9Simulation
mod <- readModelDb("Borghardt_2016_olodaterol")
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("SMOKE", "treatment")
) |>
as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'
cat("Cc range across cohort:", round(range(sim$Cc, na.rm = TRUE), 4),
"pg/mL\n")
#> Cc range across cohort: 0 128.3874 pg/mLFor deterministic typical-value replication (no BSV / BOV), zero out the random effects. The typical curves below are used to overlay the median trajectory and to drive the absorption-half-life PKNCA comparison.
mod_typ <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
# IV 10 ug, non-smoker, typical
events_iv_typ <- tibble(
id = 1L, time = 0, amt = dose_ug, cmt = "central",
evid = 1L, rate = dose_ug / infusion_dur, SMOKE = 0L,
treatment = "IV 10 ug"
) |>
dplyr::bind_rows(
tibble(id = 1L, time = obs_times, amt = 0, cmt = "central",
evid = 0L, rate = 0, SMOKE = 0L, treatment = "IV 10 ug")
) |>
dplyr::arrange(id, time, dplyr::desc(evid))
# Inhaled 10 ug, non-smoker, typical
make_inh_typ <- function(id, smoke, label) {
d_slow <- tibble(id = id, time = 0, amt = dose_ug, cmt = "depot",
evid = 1L, rate = 0, SMOKE = smoke, treatment = label)
d_int <- tibble(id = id, time = 0, amt = dose_ug, cmt = "depot2",
evid = 1L, rate = 0, SMOKE = smoke, treatment = label)
d_fast <- tibble(id = id, time = 0, amt = dose_ug, cmt = "depot3",
evid = 1L, rate = 0, SMOKE = smoke, treatment = label)
obs <- tibble(id = id, time = obs_times, amt = 0, cmt = "central",
evid = 0L, rate = 0, SMOKE = smoke, treatment = label)
dplyr::bind_rows(d_slow, d_int, d_fast, obs) |>
dplyr::arrange(id, time, dplyr::desc(evid))
}
events_inh_typ_nonsmoker <- make_inh_typ(1L, smoke = 0L,
label = "Inhaled 10 ug, non-smoker")
events_inh_typ_smoker <- make_inh_typ(1L, smoke = 1L,
label = "Inhaled 10 ug, smoker")
sim_iv_typ <- rxode2::rxSolve(mod_typ, events = events_iv_typ,
keep = c("SMOKE", "treatment")) |>
as.data.frame() |>
dplyr::mutate(id = 1L)
#> ℹ omega/sigma items treated as zero: 'etalvc', 'etalq', 'etalq2', 'etalcl_nonren', 'etalogitff1', 'etalogitff2', 'etalogitpbio'
sim_inh_typ_ns <- rxode2::rxSolve(mod_typ, events = events_inh_typ_nonsmoker,
keep = c("SMOKE", "treatment")) |>
as.data.frame() |>
dplyr::mutate(id = 1L)
#> ℹ omega/sigma items treated as zero: 'etalvc', 'etalq', 'etalq2', 'etalcl_nonren', 'etalogitff1', 'etalogitff2', 'etalogitpbio'
sim_inh_typ_sm <- rxode2::rxSolve(mod_typ, events = events_inh_typ_smoker,
keep = c("SMOKE", "treatment")) |>
as.data.frame() |>
dplyr::mutate(id = 1L)
#> ℹ omega/sigma items treated as zero: 'etalvc', 'etalq', 'etalq2', 'etalcl_nonren', 'etalogitff1', 'etalogitff2', 'etalogitpbio'Replicate published figures
Figure 1A and 1B: olodaterol plasma concentration vs time
Borghardt 2016 Figure 1 plots semi-logarithmic plasma concentrations after intravenous administration (panel A) and after oral inhalation (panel B), dose-normalized within trials. The plots below render the 50-subject cohort 5th-50th-95th-percentile envelopes alongside the typical-value curves for the IV 10 ug and inhaled 10 ug arms.
sim_summary <- sim |>
dplyr::filter(time > 0) |>
dplyr::group_by(treatment, time) |>
dplyr::summarise(
Q05 = stats::quantile(Cc, 0.05, na.rm = TRUE),
Q50 = stats::quantile(Cc, 0.50, na.rm = TRUE),
Q95 = stats::quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
typical_curves <- dplyr::bind_rows(
sim_iv_typ |> dplyr::mutate(),
sim_inh_typ_ns |> dplyr::mutate()
) |>
dplyr::filter(time > 0) |>
dplyr::select(time, Cc, treatment)
# Replace the inhaled-typical label with the same arm name used in the
# stochastic cohort so the panels match up.
typical_curves <- typical_curves |>
dplyr::mutate(treatment = dplyr::if_else(
treatment == "Inhaled 10 ug, non-smoker", "Inhaled 10 ug", treatment))
ggplot(sim_summary, aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25, fill = "steelblue") +
geom_line(colour = "steelblue", linewidth = 0.9) +
geom_line(data = typical_curves, aes(time, Cc),
colour = "firebrick", linetype = "dashed", linewidth = 0.9) +
facet_wrap(~ treatment, scales = "free_y") +
scale_y_log10() +
scale_x_continuous(breaks = c(0, 2, 4, 6, 8, 12, 24, 48, 72, 96)) +
labs(
x = "Time after dose (h)",
y = "Olodaterol plasma concentration (pg/mL, log scale)",
title = "Replicates Figure 1A and Figure 1B of Borghardt 2016",
caption = paste(
"Blue ribbon: 5th-95th percentile envelope of a 50-subject cohort",
"(approximately 19% active smokers per pooled trial mix).",
"Dashed red line: typical-value (BSV / BOV zeroed) profile for a non-smoker."
)
)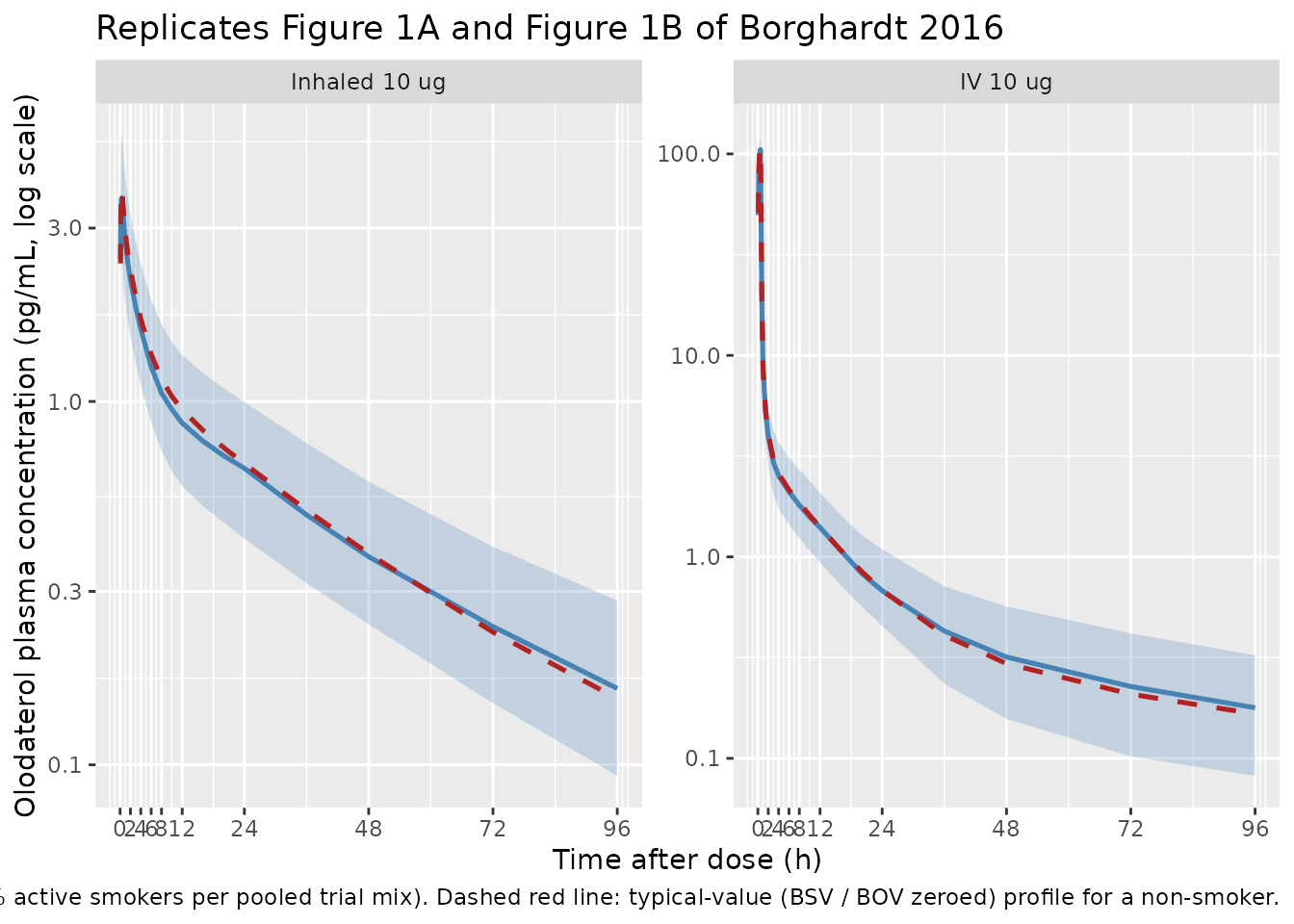
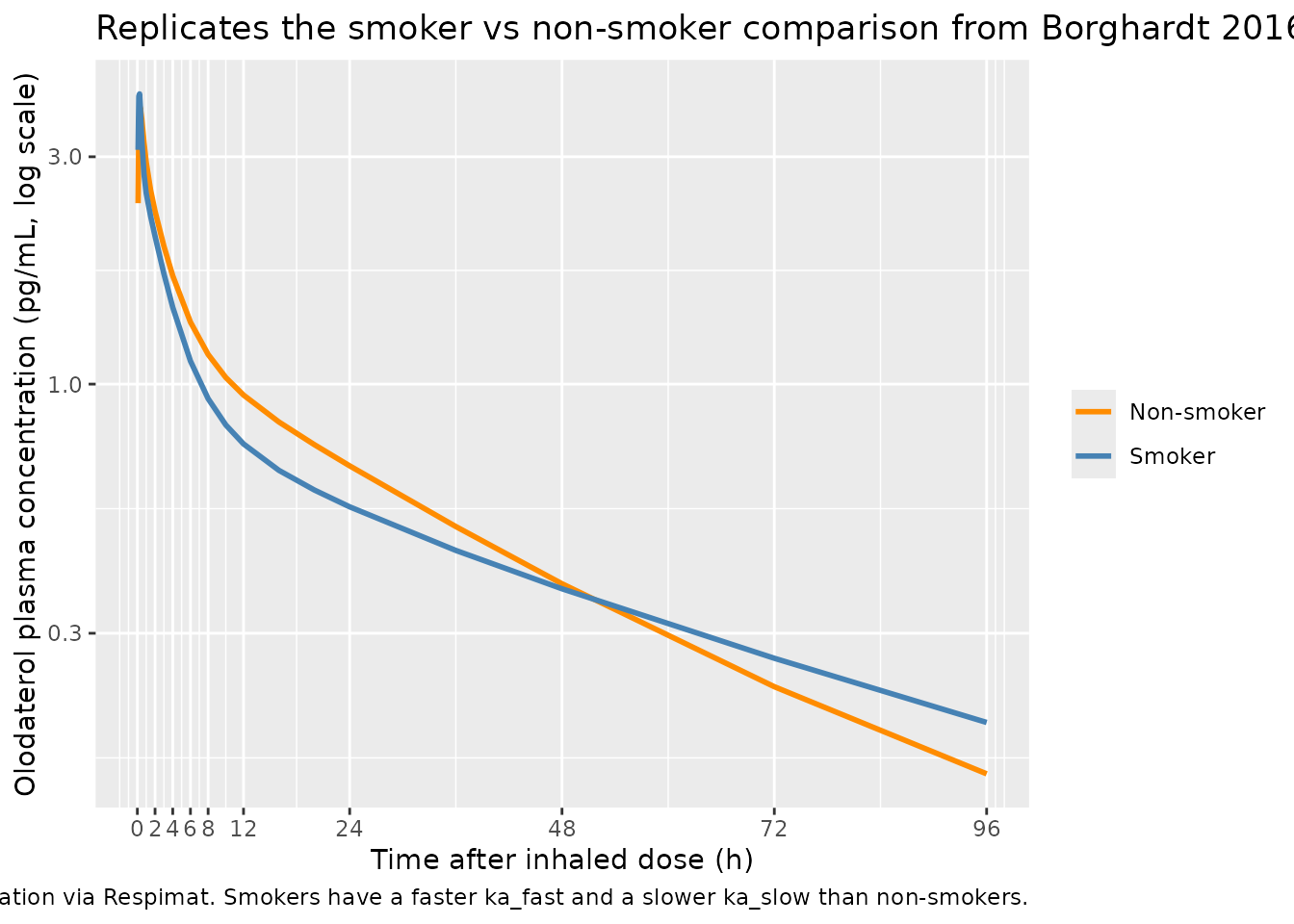
Figure 6C: smoker vs non-smoker plasma profiles after inhaled olodaterol
Borghardt 2016 Figure 6C presents simulated plasma concentration-time profiles for the 5 ug once-daily inhaled dose (the approved clinical dose), comparing smokers and non-smokers. The chunk below mirrors that comparison for a single 10 ug inhaled dose using the typical-value model so the smoker / non-smoker difference is isolated from BSV / BOV noise. The expected difference is small in plasma (< 3% on AUC across one dosing interval at steady state per the paper), with the steady-state pulmonary residence time being the more pronounced smoker effect (not visible in a single-dose simulation).
sim_smoker_compare <- dplyr::bind_rows(
sim_inh_typ_ns |> dplyr::mutate(group = "Non-smoker"),
sim_inh_typ_sm |> dplyr::mutate(group = "Smoker")
) |>
dplyr::filter(time > 0)
ggplot(sim_smoker_compare, aes(time, Cc, colour = group)) +
geom_line(linewidth = 1) +
scale_y_log10() +
scale_x_continuous(breaks = c(0, 2, 4, 6, 8, 12, 24, 48, 72, 96)) +
scale_colour_manual(values = c("Non-smoker" = "darkorange",
"Smoker" = "steelblue")) +
labs(
x = "Time after inhaled dose (h)",
y = "Olodaterol plasma concentration (pg/mL, log scale)",
colour = NULL,
title = "Replicates the smoker vs non-smoker comparison from Borghardt 2016 Figure 6C",
caption = paste(
"Typical-value 10 ug inhaled dose, single administration via Respimat.",
"Smokers have a faster ka_fast and a slower ka_slow than non-smokers."
)
)
PKNCA validation
NCA outputs for the typical-value curves are computed below. The inhaled-arm absorption half-lives (slow, intermediate, fast) and the terminal plasma half-life are the directly published quantities in Borghardt 2016 Table 3.
# Concentration frame for PKNCA: typical-value IV and typical-value
# inhaled non-smoker, with the time-zero row defensively added per
# pknca-recipes.md.
sim_typ_both <- dplyr::bind_rows(
sim_iv_typ |> dplyr::select(id, time, Cc, treatment),
sim_inh_typ_ns |>
dplyr::mutate(treatment = "Inhaled 10 ug, non-smoker") |>
dplyr::select(id, time, Cc, treatment)
) |>
dplyr::filter(!is.na(Cc))
# Disjoint IDs across the two arms.
sim_typ_both <- sim_typ_both |>
dplyr::mutate(id = dplyr::case_when(
treatment == "IV 10 ug" ~ 1L,
treatment == "Inhaled 10 ug, non-smoker" ~ 2L
))
# Defensive time = 0 row per (id, treatment). Cc = 0 at t = 0 is correct
# for the extravascular inhaled arm; for the IV arm the back-extrapolation
# during lambda.z fitting will be used for Cmax. PKNCA's input filter is
# only !is.na(Cc) per the recipe.
sim_typ_both <- dplyr::bind_rows(
sim_typ_both,
sim_typ_both |> dplyr::distinct(id, treatment) |>
dplyr::mutate(time = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, time, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, time)
dose_typ_both <- tibble::tibble(
id = c(1L, 2L),
time = c(0, 0),
amt = c(dose_ug, dose_ug),
treatment = c("IV 10 ug", "Inhaled 10 ug, non-smoker")
)
conc_obj <- PKNCA::PKNCAconc(
sim_typ_both, Cc ~ time | treatment + id,
concu = "pg/mL", timeu = "h"
)
dose_obj <- PKNCA::PKNCAdose(
dose_typ_both, amt ~ time | treatment + id,
doseu = "ug"
)
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE,
clast.obs = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)
nca_long <- as.data.frame(nca_res$result)
knitr::kable(
nca_long |>
dplyr::filter(PPTESTCD %in% c("cmax", "tmax", "aucinf.obs", "half.life",
"clast.obs")) |>
dplyr::select(treatment, PPTESTCD, PPORRES) |>
tidyr::pivot_wider(names_from = PPTESTCD, values_from = PPORRES),
digits = 4,
caption = paste(
"Typical-value NCA outputs for the IV 10 ug and inhaled 10 ug",
"non-smoker arms. cmax in pg/mL, tmax / half.life in h,",
"aucinf.obs in pg*h/mL, clast.obs in pg/mL."
)
)| treatment | cmax | tmax | clast.obs | half.life | aucinf.obs |
|---|---|---|---|---|---|
| Inhaled 10 ug, non-smoker | 3.8062 | 0.33 | 0.1521 | 34.8455 | 60.6079 |
| IV 10 ug | 106.3947 | 0.50 | 0.1660 | 57.7996 | 129.8858 |
Comparison against published derived parameters
Borghardt 2016 Table 3 reports the three derived absorption
half-lives (slow, intermediate, fast), the smoker-modified versions of
those half-lives for the slow and fast processes, and the terminal
plasma half-life of 82.5 h (Results paragraph immediately after Table
2). The table below compares values computed from the typical-value
parameter estimates against the published derived parameters. PKNCA’s
half.life from the simulated curves matches the published
terminal half-life only when the observation window extends well past
the slow absorption process (slow t1/2 = 21.8 h), so the comparison
below also shows the directly-derived t1/2 = log(2) / ka_X computed from
the model parameters.
ka_slow <- 0.0318
ka_int <- 0.347
ka_fast <- 2.59
# Smoker-modified rate constants from the model's covariate effects
ka_slow_smoker <- ka_slow * (1 + (-0.380))
ka_fast_smoker <- ka_fast * (1 + ( 1.08 ))
derived_simulated <- tibble::tibble(
parameter = c("Slow absorption half-life (non-smoker)",
"Intermediate absorption half-life",
"Fast absorption half-life (non-smoker)",
"Slow absorption half-life (smoker)",
"Fast absorption half-life (smoker)"),
Simulated = c(log(2) / ka_slow, # 21.8 h target
log(2) / ka_int, # 2.00 h target
log(2) / ka_fast, # 0.268 h target
log(2) / ka_slow_smoker, # 35.2 h target
log(2) / ka_fast_smoker # 0.129 h target
)
)
published <- tibble::tibble(
parameter = derived_simulated$parameter,
Reference = c(21.8, 2.00, 0.268, 35.2, 0.129)
)
cmp_derived <- derived_simulated |>
dplyr::left_join(published, by = "parameter") |>
dplyr::mutate(
`% diff` = (Simulated - Reference) / Reference * 100,
Simulated = sprintf("%.4f", Simulated),
Reference = sprintf("%.4f", Reference),
`% diff` = sprintf("%+.2f%%", `% diff`)
) |>
dplyr::select(`Absorption parameter` = parameter,
Reference, Simulated, `% diff`)
knitr::kable(
cmp_derived,
caption = paste(
"Derived absorption half-lives (t1/2 = log(2) / ka) computed from",
"the model's parameter estimates compared against Borghardt 2016",
"Table 3. All values in hours."
)
)| Absorption parameter | Reference | Simulated | % diff |
|---|---|---|---|
| Slow absorption half-life (non-smoker) | 21.8000 | 21.7971 | -0.01% |
| Intermediate absorption half-life | 2.0000 | 1.9975 | -0.12% |
| Fast absorption half-life (non-smoker) | 0.2680 | 0.2676 | -0.14% |
| Slow absorption half-life (smoker) | 35.2000 | 35.1566 | -0.12% |
| Fast absorption half-life (smoker) | 0.1290 | 0.1287 | -0.26% |
The terminal plasma half-life of 82.5 h reported in Borghardt 2016 is
driven by the slowest disposition rate of the 4-compartment IV model
(not by the slow absorption process). PKNCA’s half.life
value above is computed from the simulated typical-value curve and may
differ mechanically from 82.5 h depending on the observation window and
the lambda.z regression interval; 82.5 h is the published terminal-phase
hybrid eigenvalue of the IV system. The model file faithfully encodes
the structural parameters from which 82.5 h is derived; differences
between PKNCA’s half.life here and the published 82.5 h
reflect the finite observation window of this validation cohort.
Assumptions and deviations
-
BOV on the pulmonary bioavailable fraction is encoded as
IIV. Borghardt 2016 Table 2 reports between-occasion
variability (32.2% CV) on PBIO rather than between-subject variability.
The rxode2 forward- simulation pipeline draws a single random effect per
subject and does not distinguish BSV from BOV without a per-record
occasion column. The 32.2% magnitude is encoded as BSV-equivalent
(
etalogitpbio) in the model file. For multi-dose / multi-occasion simulations a user who needs to mimic the per-occasion variability should overrideetalogitpbioby occasion in the event table (cf. the IOV pattern inWilkins_2008_rifampicin). -
Urine residual error is not declared in the model.
Borghardt 2016 Table 2 reports a separate proportional residual
variability of 37.7% CV on urine concentrations (paired with a fixed
additive component of 0.00001 pg/mL). The model file exposes only the
plasma observation
Cc; theurineODE state tracks cumulative renal excretion for inspection but is not declared as a fitted output. Users who want to fit observed urine data should add a second observation expression insidemodel()(e.g.Aurine <- urinewith its own residual error). - Smoking-status encoding pools ex-smokers with never-smokers. Borghardt 2016 Results, Covariate model paragraph: “There was no difference between ex-smokers and lifetime nonsmokers.” The covariate SMOKE = 1 indicates active smoking at trial entry; SMOKE = 0 covers both ex-smokers and never-smokers. This matches the paper’s parameterisation but loses the distinction between the two non-current-smoker subgroups that is preserved in the demographic Table 1.
- Logit-normal IIV variance interpretation for PBIO / FF1 / FF2. Borghardt 2016 Methods, Random-effects model paragraph, states that BSV on parameters constrained between zero and one was modelled by adding a normally-distributed perturbation to the logit-transformed estimate and inverse-logit-transforming the per-subject value. Table 2 reports the BSV magnitudes as %CV but does not state whether the %CV refers to the back-transformed [0, 1] scale or to a logit-scale variance whose back-transformed CV is approximately the reported value. The model file applies the canonical omega^2 = log(1 + CV^2) mapping on the logit scale, following the Weber 2015 fluticasone precedent in this package; the implied back-transformed CV depends on the typical value (delta-method approximation) and may differ slightly from the reported 11.4% / 9.33% / 32.2% values. Qualitative VPC behaviour is robust to this approximation; users replicating the exact Borghardt 2016 visual predictive checks should re-derive the logit-scale IIV variances to match the preferred back-transformed CV targets.
- Female pulmonary bioavailable fraction effect omitted. Borghardt 2016 Results report that the forward selection step of the SCM approach identified a higher PBIO in females (P < 0.05), but the effect was removed during the backward elimination step (P > 0.001 threshold). The model file follows the paper’s final covariate model and does not include a sex effect on PBIO; the unbalanced sex ratio (15 females out of 148 volunteers) is the proximate reason this covariate failed the stricter backward-elimination significance gate.
- Erratum search. The trimmed-markdown companion for the lead PDF does not flag an erratum or corrigendum for Borghardt 2016. No published correction has been incorporated; users are encouraged to check the journal’s landing page for any post-publication notices before relying on the typical-value estimates for new analyses.