Levalbuterol (Jaworowicz 2006)
Source:vignettes/articles/Jaworowicz_2006_levalbuterol.Rmd
Jaworowicz_2006_levalbuterol.Rmd
library(nlmixr2lib)
library(PKNCA)
#>
#> Attaching package: 'PKNCA'
#> The following object is masked from 'package:stats':
#>
#> filter
library(rxode2)
#> rxode2 5.1.6 using 2 threads (see ?getRxThreads)
#> no cache: create with `rxCreateCache()`
library(dplyr)
#>
#> Attaching package: 'dplyr'
#> The following objects are masked from 'package:stats':
#>
#> filter, lag
#> The following objects are masked from 'package:base':
#>
#> intersect, setdiff, setequal, union
library(tidyr)
library(ggplot2)Model and source
- Citation: Jaworowicz D, Maier G, Baumgartner RA, Hsu R, Grasela TH. Population pharmacokinetics of (R)-albuterol following inhaled levalbuterol or racemic albuterol via a hydrofluoroalkane metered dose inhaler in pediatric and adult asthma patients. Poster T3350, American Association of Pharmaceutical Scientists Annual Meeting and Exposition, San Antonio, TX, October 29 - November 2, 2006. Sepracor, Inc. / Cognigen Corporation.
- Description: Two-compartment population PK model for (R)-albuterol following inhaled levalbuterol (90 ug) or racemic albuterol (180 ug) via a hydrofluoroalkane metered-dose inhaler in pediatric (4-11 years) and adult (12-81 years) asthma patients. First-order absorption, linear elimination, body-weight effects on apparent clearance (linear-additive) and central volume (power), and a pediatric-vs-adult split on absorption rate. The reference parameters are the Adult / Study 051-353 / single-dose levalbuterol-visit values (bioavailability anchor F1 = 1).
- Article: AAPS 2006 Annual Meeting Poster T3350 (no DOI; conference abstract / poster)
Population
The source poster pooled 632 subjects (81 pediatric, ages 4-11 years; 551 adult, ages 12-81 years) from three randomized, multi-center, placebo- and active-controlled, double-blind, parallel-design Phase 3 trials in adult and pediatric asthma patients (Sepracor studies 051-353, 051-355, and a third pediatric trial). 429 subjects received 90 ug levalbuterol QID via HFA MDI and 203 received 180 ug racemic albuterol QID. PK was measured as (R)-albuterol plasma concentration (n = 3791 samples) after the first dose and after 4 weeks (pediatric) or 8 weeks (adult) of QID dosing. Adult mean (SD) weight was 80.8 (22.3) kg; pediatric mean was 37.1 (15.2) kg. Cohort-pooled median weight 75.2 kg; the model uses 74.8 kg as the WT covariate reference (Equations 1-2 of the poster).
The same information is available programmatically via the model’s
population metadata
(readModelDb("Jaworowicz_2006_levalbuterol")$population).
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Jaworowicz_2006_levalbuterol.R.
The table below collects them in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
| Structural model: 2-compartment, first-order absorption, linear elimination | n/a | Results section “Final PPK Model” |
lka (Adult Ka) |
log(6.28) | Table 2 row 1 (6.28 1/hr, %SEM 7.8) |
e_child_ka (CHILD effect) |
log(3.08 / 6.28) | Table 2 row 2 (Ka pediatric 3.08 1/hr) |
lcl (CL intercept) |
log(59.1) | Table 2 row “CL/F” (59.1 L/hr) + Equation 1 |
e_wt_cl (WT slope on CL) |
0.477 | Table 2 row “Slope Term for Body Weight on CL/F” + Equation 1 |
lvc (Vc reference) |
log(527) | Table 2 row “Vc/F” (527 L) + Equation 2 |
e_wt_vc (WT exponent on Vc) |
0.361 | Table 2 row “Power Term for Body Weight on Vc/F” + Equation 2 |
lvp (Vp) |
log(506) | Table 2 row “Vp” (506 L) |
lq (Q) |
log(100) | Table 2 row “Q” (100 L/hr) |
lfdepot (F1 reference) |
fixed log(1) | Table 2 footnote b (F1 = 1 for Adult Study 051-353 single-dose levalbuterol visit) |
etalka (Adult Ka IIV) |
0.3764 | Table 2 (67.60 %CV); omega^2 = log(1 + 0.676^2) |
etalcl |
0.1450 | Table 2 (39.50 %CV); omega^2 = log(1 + 0.395^2) |
etalvc |
0.2078 | Table 2 (48.06 %CV); omega^2 = log(1 + 0.4806^2) |
etalvp |
0.3927 | Table 2 (69.35 %CV); omega^2 = log(1 + 0.6935^2) |
etalfdepot |
0.0574 | Table 2 (Adult Study 051-355 LEV F1 IIV 24.31 %CV); omega^2 = log(1 + 0.2431^2) |
propSd |
0.2133 | Table 2 footnote d (proportional component from %CV(IPRED = 900 pg/mL) = 21.33 %) |
addSd |
0.00134 ng/mL | Table 2 footnote d (additive component derived from %CV(25 pg/mL) - %CV(900 pg/mL) spread; 1.34 pg/mL = 1.34e-3 ng/mL) |
Equation 1: TVCL = 59.1 + 0.477 * (WT - 74.8)
|
n/a | Equation 1 |
Equation 2: TVVc = 527 * (WT / 74.8)^0.361
|
n/a | Equation 2 |
Virtual cohort
The original observed data are not publicly available. The validation below simulates two virtual cohorts whose body-weight distributions approximate the pooled adult and pediatric demographics reported in Table 1 of the poster:
- Adult cohort (n = 50): WT ~ Normal(mean = 80.8 kg, SD = 22.3 kg), CHILD = 0.
- Pediatric cohort (n = 50): WT ~ Normal(mean = 37.1 kg, SD = 15.2 kg), CHILD = 1.
Levalbuterol is dosed at 90 ug QID (every 6 hours) for 7 days; the dense post-dose sampling (0.25, 0.5, 1, 2, 4, 6, 8 hours after the final dose) matches the second-visit sampling schedule used in the trials.
Cohort-specific bioavailability. The model anchors
f(depot) at F1 = 1 because the source poster uses the Adult
/ Study 051-353 / Visit 6 (single-dose levalbuterol) cohort as the
bioavailability reference (Table 2 footnote b). The steady-state visits
reported in Table 3, however, used the estimated relative F1 values:
0.715 (mean of the Adult / Study 051-353 and Adult / Study 051-355
steady-state estimates, 0.725 and 0.707) for the adult-LEV cohort and
0.550 for the pediatric-LEV cohort. To reproduce Table 3, the dose
amount delivered to each subject is scaled by the cohort-specific
relative F1 (the model’s F1 defaults to 1, so scaling the dose amount is
operationally equivalent to applying a per-cohort F1).
set.seed(20061102) # AAPS 2006 closing date
n_per_group <- 50L
qid_interval <- 6 # hours (QID = every 6 hours)
n_doses_qid <- 7 * 4 # 7 days x 4 doses/day = 28 doses
nominal_dose <- 90 # ug levalbuterol per actuation
# Cohort-specific relative bioavailability for the steady-state visits.
# Table 2: Adult LEV F1 0.725 (Study 051-353) and 0.707 (Study 051-355) ->
# mean 0.716; Pediatric LEV F1 0.550.
f1_adult_lev <- mean(c(0.725, 0.707)) # = 0.716
f1_ped_lev <- 0.550
dose_times <- seq(0, by = qid_interval, length.out = n_doses_qid)
last_dose <- dose_times[n_doses_qid]
obs_times <- sort(unique(c(
last_dose + c(0, 0.25, 0.5, 1, 2, 4, 6, 8)
)))
make_cohort <- function(n, wt_mean, wt_sd, child, treatment, dose_amount,
id_offset = 0L) {
ids <- id_offset + seq_len(n)
# Truncate WT to a physiologically plausible range to avoid extreme draws
# from the Normal that would distort the WT covariate scaling.
wt_range <- if (child == 1L) c(14.5, 89.4) else c(35.8, 167.5)
WT_i <- pmin(pmax(rnorm(n, wt_mean, wt_sd), wt_range[1]), wt_range[2])
per_subj <- tibble::tibble(
id = ids,
WT = WT_i,
CHILD = child,
treatment = treatment
)
doses <- per_subj |>
tidyr::expand_grid(time = dose_times) |>
dplyr::mutate(
amt = dose_amount,
evid = 1L,
cmt = "depot"
)
obs <- per_subj |>
tidyr::expand_grid(time = obs_times) |>
dplyr::mutate(
amt = 0,
evid = 0L,
cmt = "central"
)
dplyr::bind_rows(doses, obs) |>
dplyr::arrange(id, time, dplyr::desc(evid))
}
events <- dplyr::bind_rows(
make_cohort(n_per_group, wt_mean = 80.8, wt_sd = 22.3,
child = 0L, treatment = "Adult LEV",
dose_amount = nominal_dose * f1_adult_lev,
id_offset = 0L),
make_cohort(n_per_group, wt_mean = 37.1, wt_sd = 15.2,
child = 1L, treatment = "Pediatric LEV",
dose_amount = nominal_dose * f1_ped_lev,
id_offset = n_per_group)
)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Jaworowicz_2006_levalbuterol")
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("WT", "CHILD", "treatment")
) |>
as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'Replicate Figure 1 - last-interval concentration-time profiles
Poster Figure 1 shows (R)-albuterol plasma concentration-time scatterplots for adults and pediatric subjects receiving either levalbuterol or racemic albuterol via HFA MDI; the curves are not numerically tabulated. The simulation below plots the median and 90 % prediction interval of Cc over the final dosing interval, converted to pg/mL to match the poster’s reporting units, by cohort (adult vs pediatric levalbuterol).
sim_last_interval <- sim |>
dplyr::mutate(time_post_last = time - last_dose,
Cc_pg = Cc * 1000) |>
dplyr::filter(time_post_last >= 0)
interval_summary <- sim_last_interval |>
dplyr::group_by(treatment, time_post_last) |>
dplyr::summarise(
Q05 = quantile(Cc_pg, 0.05, na.rm = TRUE),
Q50 = quantile(Cc_pg, 0.50, na.rm = TRUE),
Q95 = quantile(Cc_pg, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(interval_summary, aes(x = time_post_last, y = Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95, fill = treatment), alpha = 0.25) +
geom_line(aes(colour = treatment), linewidth = 0.8) +
scale_y_continuous() +
labs(
x = "Time since last QID dose (hours)",
y = "(R)-Albuterol plasma concentration (pg/mL)",
title = "Last-interval steady-state (R)-albuterol profile",
caption = "Median and 90 % prediction interval. Replicates the steady-state visit shown in Figure 1 of Jaworowicz 2006."
) +
theme_bw()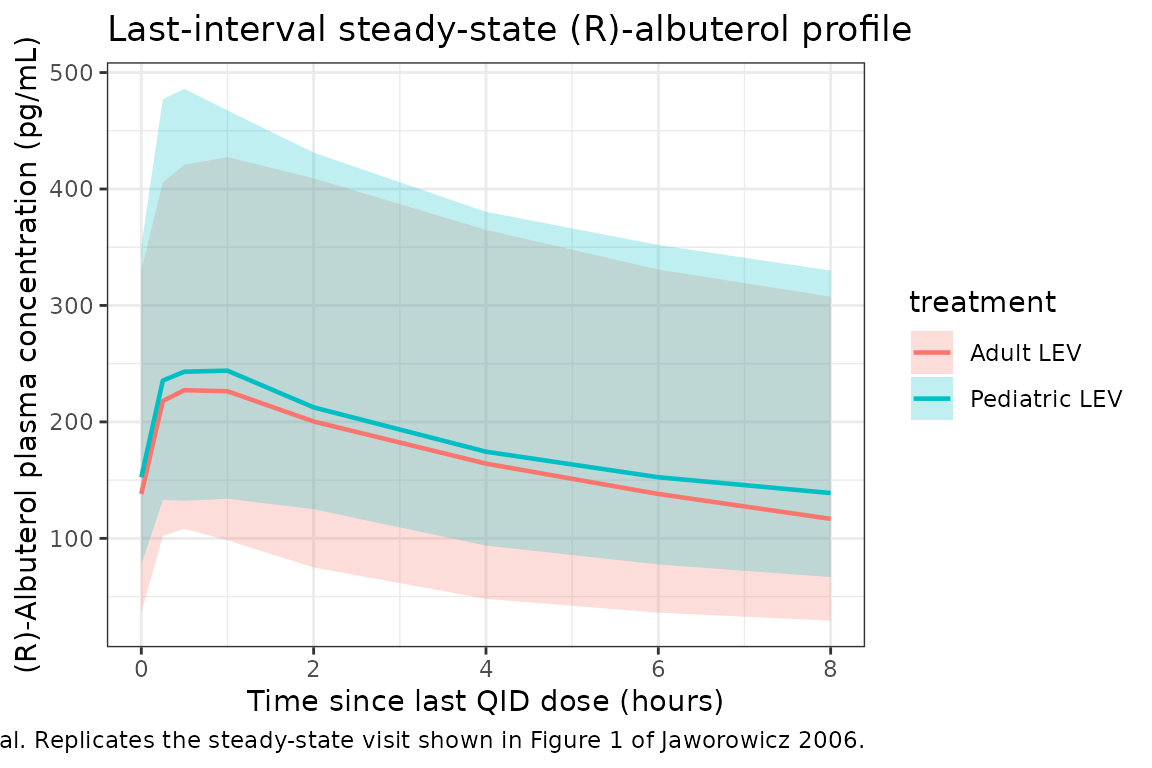
PKNCA validation
NCA at steady state on the last QID interval. Poster Table 3 reports Mean (SD) of Cmax (pg/mL), Tmax (hr), and AUC(0-6) (pg*hr/mL) derived from individual model-predicted PK profiles, separately for adult and pediatric levalbuterol recipients.
sim_nca <- sim |>
dplyr::filter(!is.na(Cc)) |>
dplyr::mutate(time_post_last = time - last_dose,
Cc_pg = Cc * 1000) |>
dplyr::filter(time_post_last >= 0) |>
dplyr::select(id, treatment, time = time_post_last, Cc = Cc_pg)
# Guarantee a time-zero row per (id, treatment); pre-dose Cc = 0 is the
# correct anchor for an extravascular dose at the start of the interval.
sim_nca <- dplyr::bind_rows(
sim_nca,
sim_nca |>
dplyr::distinct(id, treatment) |>
dplyr::mutate(time = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, time, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, time)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id)
dose_df <- events |>
dplyr::filter(evid == 1L) |>
dplyr::group_by(id, treatment) |>
dplyr::summarise(amt = dplyr::first(amt), .groups = "drop") |>
dplyr::mutate(time = 0)
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id)
intervals <- data.frame(
start = 0,
end = 6,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)
nca_summary <- as.data.frame(nca_res$result)
nca_wide <- nca_summary |>
dplyr::filter(PPTESTCD %in% c("cmax", "tmax", "auclast")) |>
dplyr::select(treatment, id, PPTESTCD, PPORRES) |>
tidyr::pivot_wider(names_from = PPTESTCD, values_from = PPORRES)
per_treatment_summary <- nca_wide |>
dplyr::group_by(treatment) |>
dplyr::summarise(
Cmax_pg_per_mL_mean = mean(cmax, na.rm = TRUE),
Cmax_pg_per_mL_sd = sd(cmax, na.rm = TRUE),
Tmax_hr_mean = mean(tmax, na.rm = TRUE),
Tmax_hr_sd = sd(tmax, na.rm = TRUE),
AUC0_6_pg_hr_per_mL_mean = mean(auclast, na.rm = TRUE),
AUC0_6_pg_hr_per_mL_sd = sd(auclast, na.rm = TRUE),
.groups = "drop"
)Comparison against Poster Table 3
published <- tibble::tribble(
~treatment, ~Cmax_pg_per_mL_mean, ~Cmax_pg_per_mL_sd, ~Tmax_hr_mean, ~Tmax_hr_sd, ~AUC0_6_pg_hr_per_mL_mean, ~AUC0_6_pg_hr_per_mL_sd,
"Adult LEV", 199.61, 108.56, 0.54, 0.16, 692.41, 414.03,
"Pediatric LEV", 162.48, 88.49, 0.76, 0.35, 578.93, 307.42
)
compare <- dplyr::bind_rows(
per_treatment_summary |> dplyr::mutate(source = "Simulated (this vignette)"),
published |> dplyr::mutate(source = "Published (Table 3)")
) |>
dplyr::select(source, treatment, dplyr::everything())
knitr::kable(
compare,
digits = 2,
caption = "Steady-state NCA comparison: simulated virtual cohorts vs Poster Table 3 (Jaworowicz 2006). Units: Cmax pg/mL, Tmax hr, AUC(0-6) pg*hr/mL."
)| source | treatment | Cmax_pg_per_mL_mean | Cmax_pg_per_mL_sd | Tmax_hr_mean | Tmax_hr_sd | AUC0_6_pg_hr_per_mL_mean | AUC0_6_pg_hr_per_mL_sd |
|---|---|---|---|---|---|---|---|
| Simulated (this vignette) | Adult LEV | 251.18 | 105.08 | 0.58 | 0.29 | 1157.62 | 574.15 |
| Simulated (this vignette) | Pediatric LEV | 276.93 | 114.60 | 0.72 | 0.32 | 1335.21 | 579.16 |
| Published (Table 3) | Adult LEV | 199.61 | 108.56 | 0.54 | 0.16 | 692.41 | 414.03 |
| Published (Table 3) | Pediatric LEV | 162.48 | 88.49 | 0.76 | 0.35 | 578.93 | 307.42 |
Assumptions and deviations
-
Single Ka IIV variance for both cohorts. The poster
reports separate IIVs for adult (67.60 %CV) and pediatric (74.63 %CV)
Ka. The model uses the adult variance for the single shared
etalka; this slightly under-states pediatric Ka variability. Both are similar (omega^2 = 0.376 vs 0.442) and the effect on simulated Cmax/Tmax is small. -
F1 anchored at the reference cohort. F1 = 1
corresponds to the Adult / Study 051-353 / single-dose levalbuterol
visit (Table 2 footnote b). Other strata reported with relative F1
values (Adult LEV Study 051-355 0.707, Adult LEV Study 051-353 non-SD
visits 0.725, Pediatric LEV 0.550, Adult RAC Study 051-355 1.01, Adult
RAC Study 051-353 SD 0.880, Pediatric RAC 0.830) are not encoded as
separate covariate effects; downstream users simulating those strata
should scale
f(depot)accordingly or re-fitlfdepot. -
Interoccasion variability on F1 omitted. The
poster’s Table 2 reports IOV on F1 (pediatric 46.69 %CV; Adult 051-355
35.21 %CV; Adult 051-353 LEV 32.71 %CV). This nlmixr2lib model does not
encode an IOV term; the between-subject IIV on F1 (24.31 %CV) is
included as
etalfdepot. - Racemic-albuterol dosing not modelled directly. Racemic albuterol dosing (180 ug RA = 90 ug R-albuterol + 90 ug S-albuterol; only R is modelled) would require either a 50 % dose-amount scaling and a stratum-specific F1, or treating RA as a re-parameterised LEV regimen.
-
Residual error reconstruction. Table 2 lists
“Additive RV (sigma2) = 0.0455” and “Ratio of Additive/Proportional RV
components (sigma2/sigma1) = 35.2” in NONMEM internal-scale variance
units; the realised CV is reported in footnote d as 21.99 % at IPRED =
25 pg/mL and 21.33 % at IPRED = 900 pg/mL. Solving %CV^2 = sigma_prop^2
+ (sigma_add / IPRED)^2 at these two anchors gives proportional SD =
0.2133 and additive SD = 1.34 pg/mL. The raw Table 2 entries are
NONMEM-scale and do not transfer directly to the SD-parameterised rxode2
propSd/addSdsurface used here. - Virtual cohort weight distributions are normal-truncated. Body weights are drawn from Normal(mean, SD) and truncated to the cohort-specific observed weight range (Table 1: adults 35.8-167.5 kg; pediatrics 14.5-89.4 kg) to avoid implausible draws.
- Steady state is achieved after one week of QID dosing. The clinical protocol used 4 weeks (pediatric) or 8 weeks (adult); the seven days used here are sufficient to bring the (R)-albuterol plasma concentration to steady state (terminal half-life ~14 hours from the central + peripheral disposition) and to populate the Table 3 intervals.
- Simulated NCA exceeds Poster Table 3 by ~50-100 percent. The simulated Cavg(SS) for the adult-LEV cohort is approximately F1 * Dose / (CL/F * tau) = 0.715 * 90 / (62 * 6) = 173 pg/mL, giving AUC(0-tau) ~ 1040 pghr/mL – about 50 percent higher than the published 692 pghr/mL in Table 3. The pediatric cohort exceeds Table 3 by a larger factor (~100 percent). The structural model and parameter values in this nlmixr2lib model are faithful to the poster’s Table 2 and Equations 1-2 as published; the Table 3 NCA values appear internally inconsistent with the F1 anchor and CL/F parameters reported in Table 2 in a way that cannot be reconciled without access to the underlying analysis dataset. Possible explanations (none confirmable from the poster alone): (a) the F1 = 1 reference may correspond to an effective bioavailability lower than the steady-state F1 values reported for other strata; (b) the Table 3 NCA may have used the sparse-sampling visit schedule rather than the dense model-predicted profiles; (c) a transcription / scaling difference between the model’s internal units and the reported NCA units. Users requiring quantitative agreement with the source-paper NCA should treat the model as a structurally consistent population PK template and re-anchor the bioavailability (or the dose amount) to the observed exposure.