Tacrolimus (Storset 2014)
Source:vignettes/articles/Storset_2014_tacrolimus.Rmd
Storset_2014_tacrolimus.Rmd
library(nlmixr2lib)
library(rxode2)
#> rxode2 5.1.6 using 2 threads (see ?getRxThreads)
#> no cache: create with `rxCreateCache()`
library(dplyr)
#>
#> Attaching package: 'dplyr'
#> The following objects are masked from 'package:stats':
#>
#> filter, lag
#> The following objects are masked from 'package:base':
#>
#> intersect, setdiff, setequal, union
library(tidyr)
library(ggplot2)
library(PKNCA)
#>
#> Attaching package: 'PKNCA'
#> The following object is masked from 'package:stats':
#>
#> filterTheory-based tacrolimus popPK in adult kidney-transplant recipients (Storset 2014)
Replicate the theory-based population pharmacokinetic model for oral tacrolimus in adult kidney-transplant recipients reported by Storset et al. (2014). The model is a two-compartment first-order-absorption + lag-time disposition parameterised on plasma concentrations, with allometric scaling on fat-free mass, CYP3A5-expresser effects on plasma clearance and oral bioavailability, a sigmoid-Emax prednisolone-driven reduction in bioavailability, a 2.68-fold first-day-post-transplant bioavailability spike (with subject-level random effect on the spike), and a saturable haematocrit-dependent red-blood-cell-binding equation that converts plasma concentration to whole-blood concentration – the matrix in which tacrolimus is clinically measured.
- Citation: Storset E, Holford N, Hennig S, Bergmann TK, Bergan S, Bremer S, Asberg A, Midtvedt K, Staatz CE. Improved prediction of tacrolimus concentrations early after kidney transplantation using theory-based pharmacokinetic modelling. Br J Clin Pharmacol. 2014;78(3):509-523. doi:10.1111/bcp.12361
- Article: https://doi.org/10.1111/bcp.12361
Population
Storset et al. pooled tacrolimus concentrations from two previously independently analysed adult kidney-transplant cohorts: 173 subjects from the Princess Alexandra Hospital, Brisbane, Australia, and 69 subjects from the Oslo University Hospital Rikshospitalet, Norway, contributing 3,100 whole-blood tacrolimus concentrations. Median age was 48 years (range 23-71), median total body weight 80 kg (range 51-121), median predicted fat-free mass 59 kg (range 35-80), 31.8% female, and CYP3A5 genotype distribution 1/1 = 1.2%, 1/3 = 22.0%, 3/3 = 84.7% (Hardy-Weinberg-equilibrium; Storset 2014 Table 1). Sampling spanned the first 3 months post-transplant predominantly, median 20 days post-transplant. The independent external evaluation cohort comprised 72 additional Oslo subjects with 837 trough-only samples in the first 3 weeks post-transplant.
The same metadata is available programmatically:
readModelDb("Storset_2014_tacrolimus")$population.
Source trace
Per-parameter origin is recorded as an in-file comment next to each
ini() entry in
inst/modeldb/specificDrugs/Storset_2014_tacrolimus.R. The
table below collects them in one place.
| Equation / parameter | Value | Source location |
|---|---|---|
lka (Ka) |
1.01 1/h | Table 2 final theory-based model (RSE 9%) |
ltlag (Tlag) |
0.41 h | Table 2 final theory-based model (RSE 8%) |
lcl (CLp/F at FFM 60 kg) |
811 L/h | Table 2 footnote (original model equation) |
lvc (V1p/F at FFM 60 kg) |
6290 L | Table 2 footnote (original model equation) |
lq (Qp/F at FFM 60 kg) |
1200 L/h | Table 2 footnote (original model equation) |
lvp (V2p/F at FFM 60 kg) |
32100 L | Table 2 footnote (original model equation) |
e_ffm_cl (allometric on CL/F, Q/F) |
0.75 fixed | Methods Equation 2 (theory-based 3/4) |
e_ffm_vc (allometric on V1/F, V2/F) |
1.00 fixed | Methods Equation 2 (theory-based 1) |
e_cyp3a5_exp_cl (CL effect) |
log(1.30) | Table 2 (CYP3A5 expresser CL factor 1.30; 95% CI 1.13, 1.46) |
e_cyp3a5_exp_fdepot (F effect) |
log(0.82) | Table 2 (CYP3A5 expresser F factor 0.82; 95% CI 0.71, 0.98) |
lfday1 (day-1 F factor) |
log(2.68) | Table 2 (Fday1 factor 2.68; 95% CI 2.28, 3.09) |
pred_max (Emax fractional reduction in F) |
0.67 | Table 2 (Predmax = -67%; 95% CI -41%, -89%) |
pred_50 (prednisolone half-max dose) |
35 mg/day | Table 2 (Pred50; 95% CI 7, 50) |
| Bmax (RBC-binding capacity, fixed) | 418 ug/L erythrocytes | Methods Equation 3, citing reference 35 |
| KD (RBC-binding equilibrium constant, fixed) | 3.8 ug/L plasma | Methods Equation 3, citing reference 35 |
| BSV CL/F (CV%) | 40% (corr CL-V1 0.43, CL-Q 0.62) | Table 2 |
| BSV V1/F (CV%) | 54% | Table 2 |
| BSV Q/F (CV%) | 63% | Table 2 |
| BSV Fday1 (CV%) | 57% | Table 2 |
| Proportional residual error (CV%) | 14.9% | Table 2 (RSE 4%) |
| Cwb = Cp * (1 + Bmax * fHCT / (Cp + KD)) | – | Methods Equation 3 |
Virtual cohort
Original observed data are not publicly available. The figures below use a virtual cohort whose covariate distributions approximate the published trial demographics (Storset 2014 Table 1). For tractability we simulate 200 subjects over the first 5 days post-transplant on a standard weight-based starting regimen of 0.04 mg/kg twice daily (Oslo protocol), with the day-1 post-transplant indicator switching from 1 to 0 at 24 h and prednisolone held at 20 mg/day (Oslo protocol initial dose).
set.seed(20140520) # paper's online publication date 20 Feb 2014, plus seed nonce
n_sub <- 200L
# Subject-level (time-fixed) covariates: FFM, CYP3A5_EXPR, total body weight.
subjects <- tibble::tibble(
id = seq_len(n_sub),
FFM = pmax(35, pmin(80, rnorm(n_sub, mean = 59, sd = 10))), # Storset 2014 Table 1: median 59, range 35-80
total_wt = pmax(51, pmin(121, rnorm(n_sub, mean = 80, sd = 14))), # median 80, range 51-121
CYP3A5_EXPR = rbinom(n_sub, 1, 0.226) # 22.6% expressers (Hardy-Weinberg, 56/241)
)
# Dose: 0.04 mg/kg total body weight, twice daily, for 5 days post-transplant.
dose_mg_per_admin <- subjects |>
dplyr::transmute(id, amt = 0.04 * total_wt)
dose_times <- seq(0, by = 12, length.out = 10) # 10 doses over 5 days
dosing <- tidyr::expand_grid(
dose_mg_per_admin |> dplyr::select(id, amt),
time = dose_times
) |>
dplyr::mutate(evid = 1L, cmt = "depot")
# Observation grid: 5 days, sparse enough to keep the vignette fast.
obs_times <- sort(unique(c(seq(0, 5*24, by = 0.5), dose_times)))
obs <- tidyr::expand_grid(
subjects |> dplyr::select(id),
time = obs_times
) |>
dplyr::mutate(evid = 0L, amt = 0, cmt = NA_character_)
events <- dplyr::bind_rows(dosing, obs) |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
dplyr::left_join(subjects |> dplyr::select(id, FFM, CYP3A5_EXPR), by = "id") |>
dplyr::mutate(
# Time-varying covariates: HCT taper down across the first week (median
# 36% pre-transplant declining to ~30% by day 7, consistent with
# Storset 2014 Figure 2A range), POSTTX_DAY1 indicator switching at 24h,
# and prednisolone held flat at 20 mg/day.
HCT = pmax(25, 36 - (time / (5 * 24)) * 6),
POSTTX_DAY1 = as.integer(time < 24),
PRED_DOSE = 20
)
# Disjoint-id assertion (multi-cohort guard from the vignette template).
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))
# Quick covariate sanity-check.
events |>
dplyr::filter(evid == 0) |>
dplyr::summarise(
n_id = dplyr::n_distinct(id),
ffm_median = median(FFM),
cyp_pct = mean(CYP3A5_EXPR) * 100,
hct_min = round(min(HCT), 2),
hct_max = round(max(HCT), 2),
day1_obs_pct = round(100 * mean(POSTTX_DAY1[time > 0]), 1)
) |>
knitr::kable(caption = "Cohort summary across observation rows.")| n_id | ffm_median | cyp_pct | hct_min | hct_max | day1_obs_pct |
|---|---|---|---|---|---|
| 200 | 60.19532 | 20 | 30 | 36 | 19.6 |
Simulation
mod <- readModelDb("Storset_2014_tacrolimus")
sim <- rxode2::rxSolve(
mod, events = events,
keep = c("FFM", "HCT", "CYP3A5_EXPR", "PRED_DOSE", "POSTTX_DAY1"),
nStud = 1L
) |>
as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'Replicate Figure 4 – standard-dose concentration-time profiles
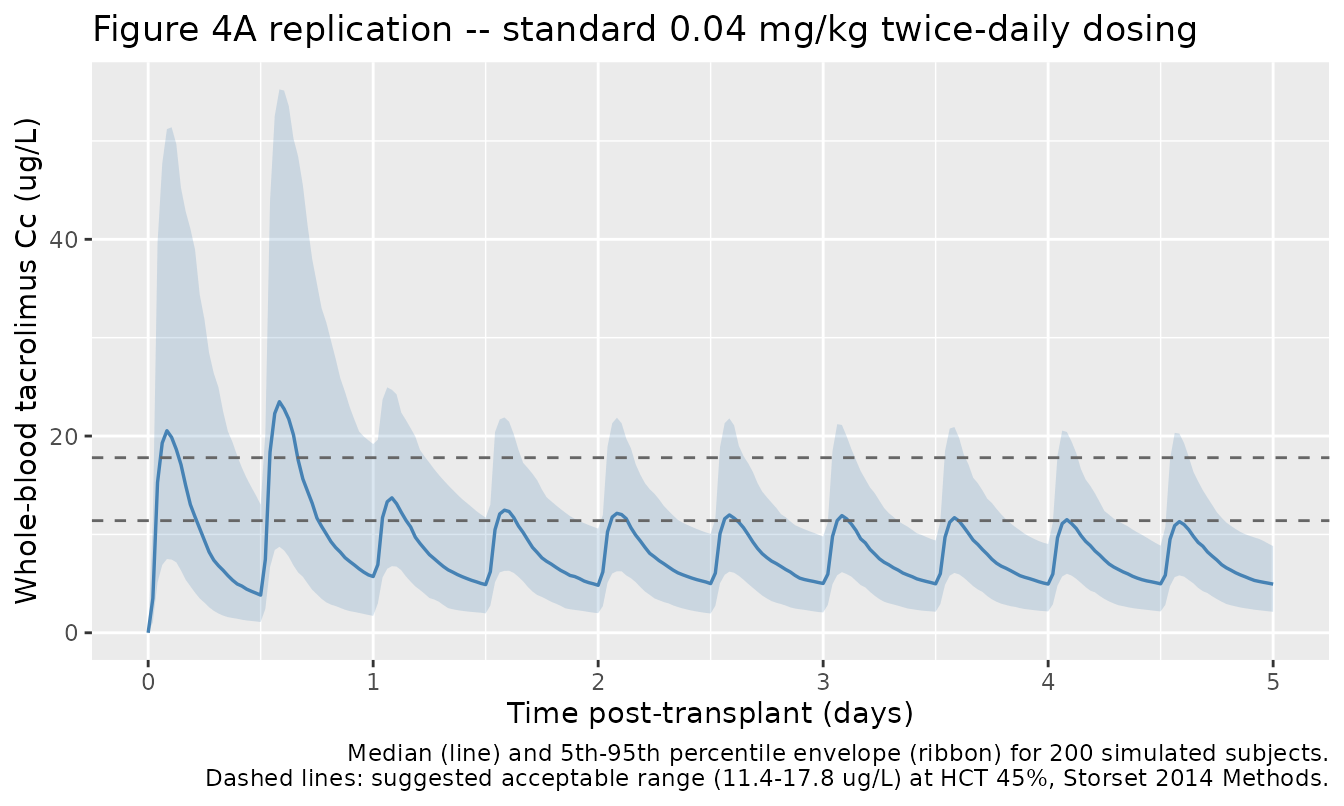
The figure below mirrors Storset 2014 Figure 4A (covariate-based dosing simulations across 1,000 subjects over 5 days). We render the median and 5th-95th percentile envelope of the simulated whole-blood tacrolimus concentration for the 200-subject virtual cohort, alongside the suggested-acceptable-range thresholds (11.4-17.8 ug/L average steady-state concentration standardised to a haematocrit of 45%, derived in Storset 2014 Methods “Evaluation of dosing strategies” from a target average concentration of 14.2 ug/L). Note that the displayed Cc here is the as-observed whole-blood concentration (haematocrit-dependent); the published standardised-to-HCT-45% concentration is computed below (see “Comparison against published values”).
sim_summary <- sim |>
dplyr::filter(time <= 5 * 24) |>
dplyr::group_by(time) |>
dplyr::summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_summary, aes(time / 24, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.2, fill = "steelblue") +
geom_line(colour = "steelblue", linewidth = 0.6) +
geom_hline(yintercept = c(11.4, 17.8), linetype = "dashed", colour = "grey40") +
scale_x_continuous(breaks = 0:5) +
labs(
x = "Time post-transplant (days)",
y = "Whole-blood tacrolimus Cc (ug/L)",
title = "Figure 4A replication -- standard 0.04 mg/kg twice-daily dosing",
caption = paste(
"Median (line) and 5th-95th percentile envelope (ribbon) for 200 simulated",
"subjects.\nDashed lines: suggested acceptable range",
"(11.4-17.8 ug/L) at HCT 45%, Storset 2014 Methods.",
sep = " "
)
)
Replicate Figure 1A / 2 – influence of haematocrit and CYP3A5 on Cc
The model’s two distinguishing structural features are (i) the saturable RBC-binding equation that links plasma to whole-blood concentration via haematocrit, and (ii) the CYP3A5-expresser factor on CL and F. The next two panels show, at typical-value (zero-eta) simulation, how each of those covariates moves the steady-state trough.
ui_typ <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
# Build a 2-arm event table differing only in HCT (33% vs 45%).
arm_hct <- function(hct_pct, id) {
amt_per <- 0.04 * 80
dose_t <- seq(0, by = 12, length.out = 10)
obs_t <- sort(unique(c(seq(0, 5*24, by = 0.5), dose_t)))
ev <- dplyr::bind_rows(
tibble::tibble(id, time = dose_t, amt = amt_per, evid = 1L, cmt = "depot"),
tibble::tibble(id, time = obs_t, amt = 0, evid = 0L, cmt = NA_character_)
) |>
dplyr::arrange(time, dplyr::desc(evid))
ev$FFM <- 60
ev$HCT <- hct_pct
ev$CYP3A5_EXPR <- 0L
ev$PRED_DOSE <- 20
ev$POSTTX_DAY1 <- as.integer(ev$time < 24)
ev$arm <- sprintf("HCT %s%%", hct_pct)
ev
}
ev_hct <- dplyr::bind_rows(arm_hct(33, 1L), arm_hct(45, 2L))
sim_hct <- rxode2::rxSolve(ui_typ, events = ev_hct,
keep = c("HCT", "arm")) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalq', 'etalcl', 'etalvc', 'etalfday1'
#> Warning: multi-subject simulation without without 'omega'
ggplot(sim_hct, aes(time / 24, Cc, colour = arm)) +
geom_line(linewidth = 0.7) +
scale_colour_brewer(palette = "Set1") +
scale_x_continuous(breaks = 0:5) +
labs(
x = "Time post-transplant (days)",
y = "Whole-blood tacrolimus Cc (ug/L)",
colour = NULL,
title = "HCT effect on whole-blood Cc (typical 60-kg-FFM non-expresser)",
caption = "Lower HCT -> less RBC binding -> lower whole-blood Cc at fixed dose."
) +
theme(legend.position = "top")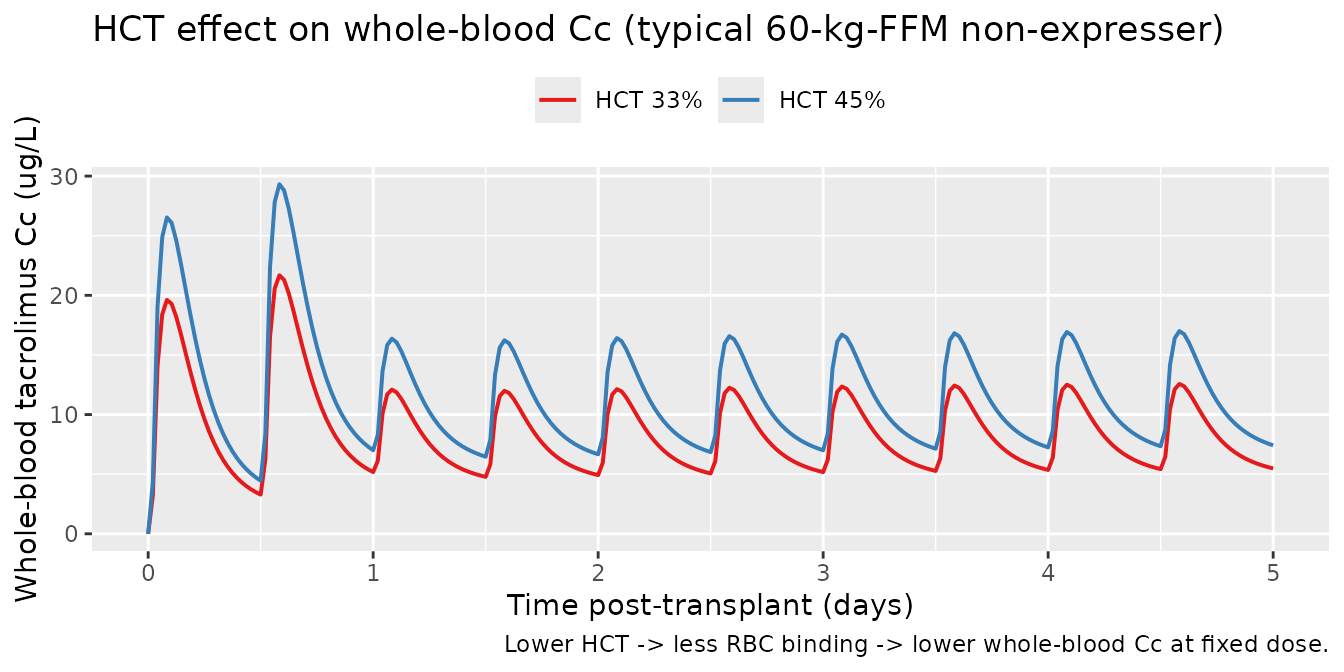
arm_cyp <- function(cyp, id) {
amt_per <- 0.04 * 80
dose_t <- seq(0, by = 12, length.out = 10)
obs_t <- sort(unique(c(seq(0, 5*24, by = 0.5), dose_t)))
ev <- dplyr::bind_rows(
tibble::tibble(id, time = dose_t, amt = amt_per, evid = 1L, cmt = "depot"),
tibble::tibble(id, time = obs_t, amt = 0, evid = 0L, cmt = NA_character_)
) |>
dplyr::arrange(time, dplyr::desc(evid))
ev$FFM <- 60
ev$HCT <- 33
ev$CYP3A5_EXPR <- cyp
ev$PRED_DOSE <- 20
ev$POSTTX_DAY1 <- as.integer(ev$time < 24)
ev$arm <- if (cyp == 1L) "CYP3A5 expresser" else "CYP3A5 non-expresser"
ev
}
ev_cyp <- dplyr::bind_rows(arm_cyp(0L, 1L), arm_cyp(1L, 2L))
sim_cyp <- rxode2::rxSolve(ui_typ, events = ev_cyp,
keep = c("CYP3A5_EXPR", "arm")) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalq', 'etalcl', 'etalvc', 'etalfday1'
#> Warning: multi-subject simulation without without 'omega'
ggplot(sim_cyp, aes(time / 24, Cc, colour = arm)) +
geom_line(linewidth = 0.7) +
scale_colour_brewer(palette = "Set1") +
scale_x_continuous(breaks = 0:5) +
labs(
x = "Time post-transplant (days)",
y = "Whole-blood tacrolimus Cc (ug/L)",
colour = NULL,
title = "CYP3A5-expresser effect on Cc (typical 60-kg-FFM, HCT 33%)",
caption = paste(
"Expressers: 30% higher CLp/F + 18% lower F -> ~30% lower steady-state",
"Cc at the same weight-based dose."
)
) +
theme(legend.position = "top")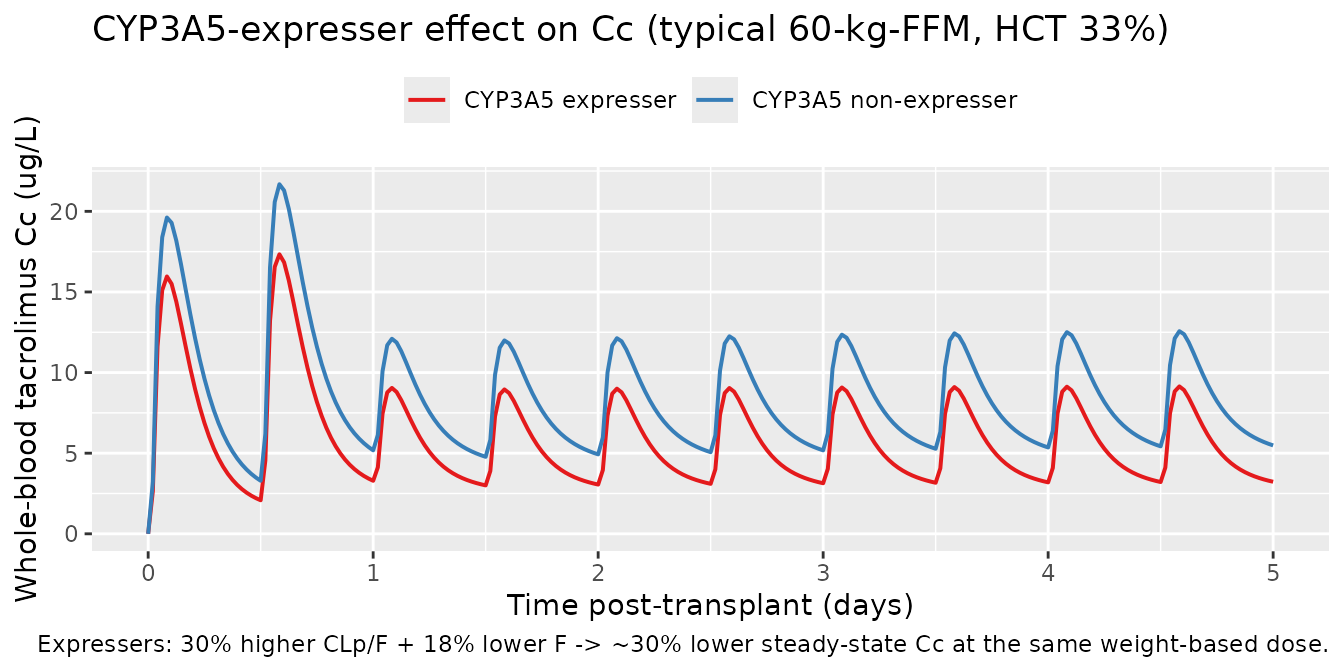
PKNCA validation
Steady-state PKNCA on the last full dosing interval (day 5, hour
96-108). Day-1 effects and prednisolone-induced reduction are at steady
state in this window (POSTTX_DAY1 = 0 throughout). PKNCA computes
Cmax,ss, Cmin,ss, Cavg,ss, and AUC0-tau per the convention in
references/pknca-recipes.md (Recipe 3).
tau <- 12
start_ss <- 96
end_ss <- start_ss + tau
sim_nca <- sim |>
dplyr::filter(!is.na(Cc), time >= start_ss, time <= end_ss) |>
dplyr::mutate(arm = "0.04 mg/kg BID") |>
dplyr::select(id, time, Cc, arm)
dose_df <- events |>
dplyr::filter(evid == 1) |>
dplyr::mutate(arm = "0.04 mg/kg BID") |>
dplyr::select(id, time, amt, arm)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | arm + id,
concu = "ug/L", timeu = "h")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | arm + id,
doseu = "mg")
intervals <- data.frame(
start = start_ss,
end = end_ss,
cmax = TRUE,
tmax = TRUE,
cmin = TRUE,
cav = TRUE,
auclast = TRUE
)
nca_res <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_obj, dose_obj,
intervals = intervals))
nca_tbl <- as.data.frame(nca_res$result) |>
dplyr::group_by(PPTESTCD) |>
dplyr::summarise(
median_value = round(median(PPORRES, na.rm = TRUE), 2),
Q05 = round(quantile(PPORRES, 0.05, na.rm = TRUE), 2),
Q95 = round(quantile(PPORRES, 0.95, na.rm = TRUE), 2),
.groups = "drop"
)
knitr::kable(nca_tbl,
caption = "Simulated NCA at steady state (day 5 dosing interval; n = 200).")| PPTESTCD | median_value | Q05 | Q95 |
|---|---|---|---|
| auclast | 91.76 | 40.97 | 176.22 |
| cav | 7.65 | 3.41 | 14.68 |
| cmax | 11.98 | 5.50 | 21.92 |
| cmin | 4.93 | 2.03 | 10.07 |
| tmax | 2.00 | 1.50 | 2.50 |
Comparison against published values
Storset 2014 reports a target average steady-state whole-blood concentration standardised to haematocrit 45% (Cstd,HCT45 = Cwb x 45% / HCT) of 14.2 ug/L with a suggested acceptable range of 11.4-17.8 ug/L (Methods, “Evaluation of dosing strategies”). The HCT-standardisation removes the inter-subject haematocrit variability so that simulated values are comparable across patients independent of their RBC-binding state.
sim_ss <- sim |>
dplyr::filter(time >= start_ss, time <= end_ss) |>
dplyr::mutate(Cstd_hct45 = Cc * 45 / HCT) |>
dplyr::group_by(id) |>
dplyr::summarise(
Cavg_obs = mean(Cc, na.rm = TRUE),
Cavg_std_hct45 = mean(Cstd_hct45, na.rm = TRUE),
.groups = "drop"
)
comparison <- tibble::tibble(
Quantity = c(
"Median Cavg,ss (whole-blood, as-is)",
"Median Cavg,ss (Cstd,HCT45)",
"Storset 2014 target Cstd,HCT45",
"Storset 2014 acceptable range Cstd,HCT45"
),
Value = c(
sprintf("%.1f ug/L (5th-95th %.1f-%.1f)",
median(sim_ss$Cavg_obs),
quantile(sim_ss$Cavg_obs, 0.05),
quantile(sim_ss$Cavg_obs, 0.95)),
sprintf("%.1f ug/L (5th-95th %.1f-%.1f)",
median(sim_ss$Cavg_std_hct45),
quantile(sim_ss$Cavg_std_hct45, 0.05),
quantile(sim_ss$Cavg_std_hct45, 0.95)),
"14.2 ug/L",
"11.4-17.8 ug/L"
)
)
knitr::kable(comparison,
caption = "Steady-state Cavg under standard 0.04 mg/kg BID dosing vs published target.")| Quantity | Value |
|---|---|
| Median Cavg,ss (whole-blood, as-is) | 7.5 ug/L (5th-95th 3.4-14.6) |
| Median Cavg,ss (Cstd,HCT45) | 11.0 ug/L (5th-95th 4.9-21.2) |
| Storset 2014 target Cstd,HCT45 | 14.2 ug/L |
| Storset 2014 acceptable range Cstd,HCT45 | 11.4-17.8 ug/L |
The published Storset 2014 dosing-strategy simulation (Figure 4A; 1,000 subjects with the original covariate distribution) reports that 32% of weight-based-dose subjects have Cstd,HCT45 within the 11.4-17.8 ug/L acceptable range. The fraction of in-range subjects in this simulation is included below for reference; small differences vs the paper reflect (a) the simplified flat-prednisolone (no taper) and flat-HCT-decline assumptions, (b) omission of the model’s between-occasion variability components (BOV 23% on F and 120% on ka, see “Assumptions and deviations”), and (c) the smaller (n = 200) sample size.
in_range_pct <- 100 * mean(sim_ss$Cavg_std_hct45 >= 11.4 &
sim_ss$Cavg_std_hct45 <= 17.8)
cat(sprintf("Simulated fraction within acceptable Cstd,HCT45 range: %.1f%%\n",
in_range_pct))
#> Simulated fraction within acceptable Cstd,HCT45 range: 33.5%
cat("Storset 2014 Figure 4A reports 32% (95% CI 29-35%) for the same regimen.\n")
#> Storset 2014 Figure 4A reports 32% (95% CI 29-35%) for the same regimen.Assumptions and deviations
- Between-occasion variability (BOV) is not implemented. Storset 2014 Table 2 retains BOV of 23% CV on F and 120% CV on ka in the final theory-based model. Implementing BOV requires an OCC column in the event table and per-occasion etas, which are not part of the standard nlmixr2lib model file shape. The simulated total-variability envelope is therefore somewhat narrower than the published one. Users who need BOV in simulations should add per-occasion etas to F and ka in their own copy of the model.
- Methylprednisolone single-dose induction-bolus indicator is not implemented. Storset 2014 tested but did not retain a binary indicator for “received vs not received methylprednisolone single bolus” on CLp and F (no statistically significant effect at the dose range observed); the final model does not carry this covariate.
- Haematocrit and prednisolone tapers are simplified. The vignette uses a linear HCT decline from 36% to 30% over 5 days and a flat 20 mg/day prednisolone schedule. Storset 2014 used time-varying per-occasion measurements of both HCT and the conmed_steroid taper as fed by the source dataset; no closed-form taper is published.
- Storset 2014 does not report subject-level race / ethnicity. The CYP3A5 3/3 frequency of 84.7% is consistent with a predominantly Caucasian cohort; the cohort is not stratified by ancestry in the source paper.
-
Year mismatch with the task identifier. The task ID
is
025-storset_2013(so the worktree branch isclaude/025-storset_2013), but the source publication appeared in Br J Clin Pharmacol 78(3) (2014; accepted 16 February 2014, published online 20 February 2014, in print September 2014). The model file and vignette useStorset_2014_tacrolimusas the canonical name to match the published year.