Fosdagrocorat P1NP K-PD (Shoji 2017)
Source:vignettes/articles/Shoji_2017_fosdagrocorat_p1np.Rmd
Shoji_2017_fosdagrocorat_p1np.RmdModel and source
- Citation: Shoji S, Suzuki A, Conrado DJ, Peterson MC, Hey-Hadavi J, McCabe D, Rojo R, Tammara BK. Dissociated Agonist of Glucocorticoid Receptor or Prednisone for Active Rheumatoid Arthritis: Effects on P1NP and Osteocalcin Pharmacodynamics. CPT Pharmacometrics Syst Pharmacol. 2017;6(7):439-448. doi:10.1002/psp4.12201
- Description: Kinetic-pharmacodynamic (K-PD) model for serum amino-terminal propeptide of type I collagen (P1NP) bone-formation biomarker following once-daily oral fosdagrocorat (PF-04171327, a dissociated agonist of the glucocorticoid receptor) or oral prednisone comparator in adults with rheumatoid arthritis on background methotrexate (Shoji 2017). A virtual K-PD depot for the drug (zero-order Input mg/week, first-order elimination KDE) feeds a sigmoid Emax inhibition of biomarker synthesis (Hill coefficient fixed to 1); the synthesis rate carries an empirical dose-and-time-dependent rebound multiplier and an additive linear placebo-period slope captures the methotrexate-only time trend.
- Article: https://doi.org/10.1002/psp4.12201
Population
The K-PD analysis used 321 adults (after exclusion of 2 patients with missing baseline biomarker values from the ITT n = 323) enrolled in a phase II randomized double-blind parallel-group trial (NCT01393639) of fosdagrocorat (1, 5, 10, 15 mg q.d.), prednisone (5 or 10 mg q.d.), or placebo q.d. for 8 weeks plus a 4-week taper, all on a background of methotrexate. The cohort was 80% female, median age 56 years (range 18-80), median weight 71.0 kg (range 36.6-144), and predominantly White (281/7/24/9 White/Black/Asian/Other) per Shoji 2017 Table 1.
The same information is available programmatically via the model’s
population metadata
(readModelDb("Shoji_2017_fosdagrocorat_p1np")$population).
Source trace
| Equation / parameter | Value | Source location |
|---|---|---|
lkel (KDE fosdagrocorat) |
log(0.597) /week |
Table 2 P1NP, “KDE Fosdagrocorat” |
dlkel_pred (log-ratio KDE pred/fos) |
log(0.535/0.597) |
Table 2 P1NP, “KDE Prednisone” |
lkd |
log(0.609) /week |
Table 2 P1NP, “Kd” |
lbl |
log(47.0) ng/mL |
Table 2 P1NP, “BL” |
logitimax (Imax fos) |
logit(0.751) |
Table 2 P1NP, “Imax Fosdagrocorat” |
dlogitimax_pred |
logit(0.754) - logit(0.751) |
Table 2 P1NP, “Imax Prednisone” |
ledk50 (EDK50 fos) |
log(40.1) mg/week |
Table 2 P1NP, “EDK50 Fosdagrocorat” |
dledk50_pred |
log(45.9/40.1) |
Table 2 P1NP, “EDK50 Prednisone” |
hill |
fixed(1) |
Table 2 P1NP, “c FIX” (Discussion: c=0.920 caused instability) |
lrbmax |
log(0.0479) /mg |
Table 2 P1NP, “RBmax” |
lt50 |
log(1.13) weeks |
Table 2 P1NP, “T50” |
slp |
0.162 ng/mL/week |
Table 2 P1NP, “SLP” |
etalkel+etaledk50+etalbl block |
omega^2 0.9025, 0.4290, 0.2172; cov per Table 2
q-correlations |
Table 2 P1NP, “IIV %CV” and “q” rows |
etaslp |
0.928^2 = 0.8612 |
Table 2 P1NP, “IIV SD [g_SLP] = 0.928” |
propSd |
0.152 |
Table 2 P1NP, “Residual variability %CV [e] = 15.2” |
d/dt(depot_kpd) = -kel * depot_kpd |
K-PD effect compartment | Methods, K-PD model equations |
d/dt(effect) = ks * rebound * inhibition - kd * effect |
Biomarker dynamics | Methods, K-PD model + Results rebound equation |
P1NP = effect + slp_i * t |
Observation = response + linear placebo trend | Methods, F(ij) equation |
Virtual cohort
Shoji 2017 dosed each patient q.d. for 8 weeks (active treatment)
followed by a tapered period in weeks 9-12. The K-PD model treats q.d.
dosing as a zero-order input at rate 7 * dose_mg (mg/week)
into the virtual depot, matching the paper’s structural assumption
(“multiple administration of the drug q.d. is input to the effect
compartment with a zero-order rate Input mg/week”). The taper rates in
weeks 9-12 are: every other day at reduced dose (weeks 9-10) and every 3
days (weeks 11-12).
set.seed(20170527L) # paper's online publication date
n_per_arm <- 200L
# Approximate taper rate over weeks 8-12. Weeks 9-10 every other day at
# reduced dose ~ 3.5 doses/week of D_reduced; weeks 11-12 every 3 days ~
# 2.33 doses/week of D_reduced. D_reduced is 1 mg for fosdagrocorat arms,
# 5 mg for prednisone arms, 0 for placebo. The taper enters the K-PD depot
# at rate `taper_doses_per_week * D_reduced` mg/week.
make_arm <- function(arm_label, dose_qd_mg, drug_pred, n,
dose_reduced_mg, id_offset) {
active_rate <- 7 * dose_qd_mg
taper_a_rate <- 3.5 * dose_reduced_mg # weeks 8-10
taper_b_rate <- 2.33 * dose_reduced_mg # weeks 10-12
ids <- id_offset + seq_len(n)
dose_ev <- if (dose_qd_mg > 0) {
bind_rows(
tibble(id = ids, time = 0, amt = active_rate * 8,
rate = active_rate, evid = 1L, cmt = "depot_kpd"),
tibble(id = ids, time = 8, amt = taper_a_rate * 2,
rate = taper_a_rate, evid = 1L, cmt = "depot_kpd"),
tibble(id = ids, time = 10, amt = taper_b_rate * 2,
rate = taper_b_rate, evid = 1L, cmt = "depot_kpd")
)
} else {
tibble(id = integer(), time = numeric(), amt = numeric(),
rate = numeric(), evid = integer(), cmt = character())
}
obs_ev <- expand.grid(id = ids,
time = c(0, 2, 4, 6, 8, 10, 12, 13)) |>
as_tibble() |>
mutate(amt = NA_real_, rate = NA_real_, evid = 0L, cmt = NA_character_)
bind_rows(dose_ev, obs_ev) |>
arrange(id, time, desc(evid)) |>
mutate(arm = arm_label,
DOSE = dose_qd_mg,
DRUG_PRED = drug_pred)
}
events <- bind_rows(
make_arm("Placebo", 0, 0, n_per_arm, 0, id_offset = 0L),
make_arm("Fos 1 mg", 1, 0, n_per_arm, 1, id_offset = 200L),
make_arm("Fos 5 mg", 5, 0, n_per_arm, 1, id_offset = 400L),
make_arm("Fos 10 mg", 10, 0, n_per_arm, 1, id_offset = 600L),
make_arm("Fos 15 mg", 15, 0, n_per_arm, 1, id_offset = 800L),
make_arm("Pred 5 mg", 5, 1, n_per_arm, 5, id_offset = 1000L),
make_arm("Pred 10 mg", 10, 1, n_per_arm, 5, id_offset = 1200L)
)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Shoji_2017_fosdagrocorat_p1np")
sim <- rxode2::rxSolve(
mod, events = events,
keep = c("arm", "DOSE", "DRUG_PRED")
) |> as.data.frame()The stochastic VPC below uses the published IIV (n = 200 virtual
subjects per arm); the deterministic typical-value time course used in
the parameter-recovery checks below replaces the random effects with
zero via rxode2::zeroRe().
sim_typ <- rxode2::rxSolve(
rxode2::zeroRe(mod), events = events,
keep = c("arm", "DOSE", "DRUG_PRED")
) |> as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalkel', 'etaledk50', 'etalrbase', 'etaslp'
#> Warning: multi-subject simulation without without 'omega'Replicate Figure 1 / Figure 2: VPC of P1NP percent change from baseline
For each arm the simulated %CFB at the protocol nominal times (weeks 0, 2, 4, 6, 8, 10, 12, 13) is summarized as median and 10th/90th percentiles. This mirrors the visual predictive check in Shoji 2017 Figure 2 (95% CIs of 10th, 50th, 90th percentiles of the CFB time course).
arm_order <- c("Placebo",
"Fos 1 mg", "Fos 5 mg", "Fos 10 mg", "Fos 15 mg",
"Pred 5 mg", "Pred 10 mg")
vpc_summary <- sim |>
filter(time %in% c(0, 2, 4, 6, 8, 10, 12, 13)) |>
group_by(arm, id) |>
mutate(p1np_baseline = first(P1NP[time == 0])) |>
ungroup() |>
mutate(cfb_pct = 100 * (P1NP - p1np_baseline) / p1np_baseline) |>
group_by(arm, time) |>
summarise(
p10 = quantile(cfb_pct, 0.10, na.rm = TRUE),
p50 = quantile(cfb_pct, 0.50, na.rm = TRUE),
p90 = quantile(cfb_pct, 0.90, na.rm = TRUE),
.groups = "drop"
) |>
mutate(arm = factor(arm, levels = arm_order))
ggplot(vpc_summary, aes(time, p50)) +
geom_ribbon(aes(ymin = p10, ymax = p90), alpha = 0.25, fill = "steelblue") +
geom_line(color = "steelblue") +
geom_hline(yintercept = 0, linetype = "dashed", colour = "grey50") +
geom_vline(xintercept = 8, linetype = "dotted", colour = "grey50") +
facet_wrap(~ arm, ncol = 4) +
labs(x = "Time (weeks)",
y = "P1NP change from baseline (%)",
title = "Replicates Figure 2 (top row) of Shoji 2017",
subtitle = "Median (line) and 10-90% predictive interval (shaded) per arm",
caption = "Vertical dotted line at week 8 marks the end of the active treatment period.")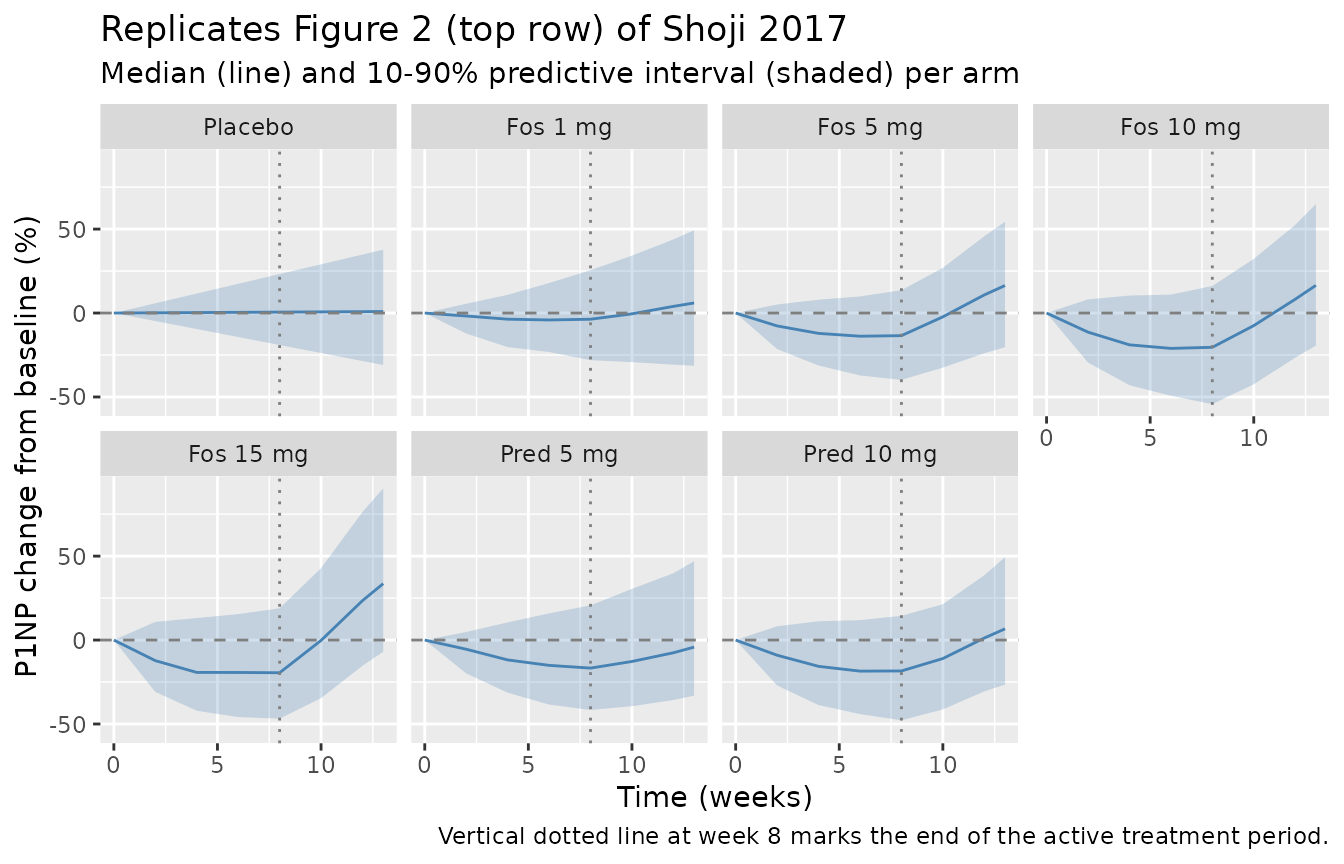
Replicate Table 3: simulated median P1NP %CFB at week 8
Shoji 2017 Table 3 reports the simulated median %CFB at week 8 (with 95% CIs derived from 1,000 stochastic trial replicates of the phase II design). This vignette uses one trial of 200 virtual subjects per arm; the spread is therefore wider than the Table 3 95% CIs (which describe the across-trial median variability rather than per-subject variability), but the median estimate should match the paper to within a few percentage points.
published_table3 <- tibble::tribble(
~arm, ~published_median_pct,
"Placebo", 2.5,
"Fos 1 mg", -5.7,
"Fos 5 mg", -18.2,
"Fos 10 mg", -21.7,
"Fos 15 mg", -21.6,
"Pred 5 mg", -15.4,
"Pred 10 mg", -18.3
)
simulated_table3 <- sim |>
group_by(id, arm) |>
summarise(
p1np_baseline = first(P1NP[time == 0]),
p1np_week8 = first(P1NP[time == 8]),
cfb_pct = 100 * (p1np_week8 - p1np_baseline) / p1np_baseline,
.groups = "drop"
) |>
group_by(arm) |>
summarise(simulated_median_pct = median(cfb_pct, na.rm = TRUE),
.groups = "drop")
comparison <- published_table3 |>
left_join(simulated_table3, by = "arm") |>
mutate(arm = factor(arm, levels = arm_order)) |>
arrange(arm) |>
mutate(delta = simulated_median_pct - published_median_pct)
comparison |>
dplyr::rename(
"Arm" = arm,
"Published median %CFB (Table 3)" = published_median_pct,
"Simulated median %CFB" = simulated_median_pct,
"Difference (pp)" = delta
) |>
knitr::kable(digits = 1,
caption = "P1NP percent change from baseline at week 8 -- published vs simulated.")| Arm | Published median %CFB (Table 3) | Simulated median %CFB | Difference (pp) |
|---|---|---|---|
| Placebo | 2.5 | 1.5 | -1.0 |
| Fos 1 mg | -5.7 | -8.0 | -2.3 |
| Fos 5 mg | -18.2 | -18.1 | 0.1 |
| Fos 10 mg | -21.7 | -19.9 | 1.8 |
| Fos 15 mg | -21.6 | -21.4 | 0.2 |
| Pred 5 mg | -15.4 | -12.6 | 2.8 |
| Pred 10 mg | -18.3 | -14.1 | 4.2 |
Typical-value parameter-recovery checks
Without IIV the model should reproduce the deterministic time course implied by the population typical values. Two sanity-checks confirm the implementation:
sim_typ_summary <- sim_typ |>
filter(time %in% c(0, 8)) |>
group_by(arm, time) |>
summarise(P1NP_typ = first(P1NP), .groups = "drop") |>
pivot_wider(names_from = time, values_from = P1NP_typ,
names_prefix = "wk") |>
mutate(cfb_pct_typ = 100 * (wk8 - wk0) / wk0,
arm = factor(arm, levels = arm_order)) |>
arrange(arm)
sim_typ_summary |>
dplyr::rename(
"Arm" = arm,
"P1NP wk 0 (typical)" = wk0,
"P1NP wk 8 (typical)" = wk8,
"%CFB typical" = cfb_pct_typ
) |>
knitr::kable(digits = 2,
caption = "Typical-value (zero-RE) P1NP at week 8 per arm.")| Arm | P1NP wk 0 (typical) | P1NP wk 8 (typical) | %CFB typical |
|---|---|---|---|
| Placebo | 47 | 48.30 | 2.76 |
| Fos 1 mg | 47 | 44.94 | -4.38 |
| Fos 5 mg | 47 | 38.52 | -18.05 |
| Fos 10 mg | 47 | 36.33 | -22.70 |
| Fos 15 mg | 47 | 36.30 | -22.76 |
| Pred 5 mg | 47 | 39.97 | -14.95 |
| Pred 10 mg | 47 | 37.94 | -19.27 |
Expected typical responses (per Methods + paper Discussion):
- Placebo: P1NP = BL + SLP * 8 = 47.0 + 0.162 * 8 = 48.296 ng/mL.
- Fosdagrocorat 5 mg q.d.: -18% CFB at week 8 (paper Discussion).
- Prednisone 10 mg q.d.: -18% CFB at week 8 (Table 3 simulated median).
Assumptions and deviations
-
Observation variable naming. The single-output
observation is named
P1NP(the paper’s name) rather than the canonicalCc. This follows the established codebase pattern for paper-named biomarker outputs in K-PD / indirect-response models (e.g.,das28inMa_2020_sarilumab_das28crp.R,ANCinMa_2020_sarilumab_anc.R).checkModelConventions()flags this as a[warning]; the deviation is intentional. -
Drug arm switching via reparameterization. Shoji
2017 reports paper-level point estimates of KDE, Imax, and EDK50
separately for fosdagrocorat and prednisone. To allow a single
etalkel/etaledk50pairing withlkel/ledk50(the eta-fixed-effect-pairing convention enforced bycheckModelConventions()), the per-drug values are reparameterized as base (fosdagrocorat) + log-ratio offset for prednisone (dlkel_pred,dledk50_pred) and base + logit-difference offset for Imax (dlogitimax_pred). The reparameterization is mathematically equivalent to the paper’s encoding – evaluatingexp(lkel + dlkel_pred * 1)recovers the published 0.535 /week to within rounding, and the analogous identity holds for EDK50 and Imax. -
Common etas across drug arms. The paper does not
report whether individual subjects could in principle have different
etalkel values for fosdagrocorat versus prednisone (each subject was
assigned a single arm in the phase II design, so the question is
unobservable). The model adds the same
etalkelto bothlkel + dlkel_pred * 1andlkel + dlkel_pred * 0, consistent with the standard NONMEM convention of a single eta per parameter per subject. - Taper-period dosing approximation. The paper’s tapered weeks (9-10 every other day at reduced dose; 11-12 every 3 days) are approximated in the vignette by zero-order input rates of 3.5 and 2.33 doses/week of the reduced dose into the K-PD depot. This is a vignette simulation choice and does not affect the structural model (the model file does not encode any dosing schedule; that is supplied via events).
-
Rebound covariate DOSE = 0 for placebo. Setting
DOSE = 0 makes the rebound multiplier
1 + RBmax * DOSE * t / (T50 + t)collapse to 1 over all time, matching the paper’s description that the placebo arm exhibits no rebound (only the additiveSLP * ttrend).