Remifentanil (Yang 2017)
Source:vignettes/articles/Yang_2017_remifentanil.Rmd
Yang_2017_remifentanil.RmdModel and source
- Citation: Yang S, Noh H, Hahn J, Jin BH, Min KL, Bae SK, Kim J, Park MS, Hong T, Wi J, Chang MJ. Population pharmacokinetics of remifentanil in critically ill patients receiving extracorporeal membrane oxygenation. Sci Rep 2017;7(1):16275. doi:10.1038/s41598-017-16358-6.
- Description: One-compartment population PK model for continuous intravenous remifentanil infusion in critically ill adults receiving venoarterial extracorporeal membrane oxygenation (VA-ECMO), with sex and centrifugal-pump rotational speed as covariates on clearance (Yang 2017).
- Article: https://doi.org/10.1038/s41598-017-16358-6 (open access in Scientific Reports 2017;7:16275)
Population
Yang et al. enrolled 15 critically ill adults (median age 57 years,
IQR 45-69; 67% male; median weight 65.4 kg, IQR 54.5-70.0; median BMI
23.8 kg/m^2) receiving continuous-infusion remifentanil sedation during
venoarterial extracorporeal membrane oxygenation (VA-ECMO) at Severance
Cardiovascular Hospital, Yonsei University (Seoul, South Korea), between
January 2015 and December 2016 (ClinicalTrials.gov NCT02581280;
single-center prospective cohort). Indications for VA-ECMO were
predominantly acute coronary syndromes (acute MI n = 5, NSTEMI n = 4,
STEMI n = 1, ischemic cardiomyopathy n = 1) with several other
cardiopulmonary failures (pulmonary embolism, coronary artery occlusive
disease, myocarditis, atrial fibrillation with bronchiolitis, angina
pectoris). Median ECMO support duration was 143 h (IQR 96-250). Median
centrifugal-pump rotational speed was 2350 RPM (IQR 2302-2532). Ten of
the 15 patients (67%) received concomitant CRRT during ECMO support;
CRRT was tested as a covariate during model development but not retained
in the final model. Baseline characteristics are listed in Table 1 of
the source paper. The same information is available programmatically via
readModelDb("Yang_2017_remifentanil")()$meta$population.
Source trace
Per-parameter origin is recorded as an in-file comment next to each
ini() entry in
inst/modeldb/specificDrugs/Yang_2017_remifentanil.R. The
table below collects the equations and parameter values in one place for
review.
| Equation / parameter | Value | Source location |
|---|---|---|
| One-compartment model with zero-order input and first-order elimination | n/a | Results, paragraph 2; Methods, Structural and model development |
| Final CL model: CL (L/h) = 366 x 0.502^SEX x (ECMO pump speed / 2350)^2.04, with SEX = 0 (female), 1 (male) | n/a | Results, Population PK analysis (final-model equation) |
lcl (typical female CL at 2350 RPM) |
366 L/h | Table 2 (theta_CL) |
lvc (typical V) |
41 L | Table 2 (theta_V) |
e_sex_cl (log(0.502); applied via (1 - SEXF) to
preserve female reference) |
-0.6892 | Table 2 (theta_sex on CL = 0.502) |
e_pumpspeed_cl (power exponent on ECMO pump speed /
2350) |
2.04 | Table 2 (theta_ECMOpumpspeed on CL) |
etalcl (IIV variance on log CL; stored as SD^2 =
0.124^2) |
0.01538 | Table 2 (omega_CL = 0.124, SD on log scale) |
propSd (proportional residual SD, fraction) |
0.387 | Table 2 (sigma_proportional = 0.387) |
addSd (additive residual SD, ng/mL) |
0.111 ng/mL | Table 2 (sigma_additive = 0.111 ng/mL) |
| Reference pump speed (median of cohort) | 2350 RPM | Results, Patient characteristics; Table 1 |
Virtual cohort
Original observed concentrations are not publicly available. The figures below use a virtual cohort that mirrors the simulation grid used in the source paper (Methods, Simulations; Results, Predicted concentration profiles; Figure 4):
- Sex: female (
SEXF = 1) and male (SEXF = 0). - ECMO pump speed: 1700, 2000, 2300, 2600, and 2900 RPM (Yang 2017 Methods, Simulations).
- Remifentanil infusion rates: 0.105, 0.21, 0.42, 0.63, and 0.84 mg/h (= 105, 210, 420, 630, 840 ug/h). The infusion is continuous over 48 h, matching the paper’s two-day simulation horizon.
set.seed(2017)
pump_speeds_rpm <- c(1700, 2000, 2300, 2600, 2900)
infusion_rates_mg_h <- c(0.105, 0.21, 0.42, 0.63, 0.84)
sexes <- c(Female = 1L, Male = 0L)
n_per_group <- 25L # virtual subjects per (sex, pump speed, dose) group
inf_duration_h <- 48 # 2-day continuous infusion (Methods, Simulations)
obs_times <- seq(0, 48, by = 2)
make_cohort <- function(n, sex_label, sexf_val, pump_rpm, dose_mg_h, id_offset) {
rate_ug_h <- dose_mg_h * 1000 # mg/h -> ug/h (model dose units are ug)
amt_ug <- rate_ug_h * inf_duration_h
per_subject <- function(sid) {
dplyr::bind_rows(
data.frame(id = sid, time = 0, amt = amt_ug, rate = rate_ug_h,
evid = 1L, cmt = "central",
SEXF = sexf_val,
ECMO_PUMP_SPEED = pump_rpm,
sex_label = sex_label,
pump_rpm = pump_rpm,
dose_mg_h = dose_mg_h),
data.frame(id = sid, time = obs_times, amt = NA_real_, rate = NA_real_,
evid = 0L, cmt = NA_character_,
SEXF = sexf_val,
ECMO_PUMP_SPEED = pump_rpm,
sex_label = sex_label,
pump_rpm = pump_rpm,
dose_mg_h = dose_mg_h)
)
}
ids <- id_offset + seq_len(n)
do.call(rbind, lapply(ids, per_subject))
}
# Build a grid: 2 sex x 5 pump speeds x 5 doses = 50 groups
grid <- tidyr::expand_grid(
sex_label = names(sexes),
pump_rpm = pump_speeds_rpm,
dose_mg_h = infusion_rates_mg_h
)
grid$id_offset <- (seq_len(nrow(grid)) - 1L) * n_per_group
events <- do.call(rbind, lapply(seq_len(nrow(grid)), function(i) {
row <- grid[i, ]
make_cohort(
n = n_per_group,
sex_label = row$sex_label,
sexf_val = sexes[[row$sex_label]],
pump_rpm = row$pump_rpm,
dose_mg_h = row$dose_mg_h,
id_offset = row$id_offset
)
}))
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))
events$cohort <- paste0(events$sex_label,
" / ", events$pump_rpm, " RPM / ",
events$dose_mg_h, " mg/h")Simulation
mod <- readModelDb("Yang_2017_remifentanil")()
sim <- rxode2::rxSolve(
mod, events = events, addCov = TRUE,
keep = c("sex_label", "pump_rpm", "dose_mg_h", "cohort")
)
sim <- as.data.frame(sim)Replicate Figure 4 – simulated remifentanil concentrations by sex x pump speed x dose
The paper’s Figure 4 shows simulated mean remifentanil concentrations in female and male patients across the 5 pump speeds (1700, 2000, 2300, 2600, 2900 RPM) for 5 infusion rates (0.84, 0.63, 0.42, 0.21, 0.105 mg/h). The horizontal reference line at 1.5 ng/mL is the sedation target referenced in the paper (Discussion; “a target concentration >= 1.5 ng/mL”).
fig4 <- sim |>
dplyr::filter(!is.na(Cc), time > 0) |>
dplyr::group_by(sex_label, pump_rpm, dose_mg_h, time) |>
dplyr::summarise(
median_Cc = median(Cc, na.rm = TRUE),
p05 = quantile(Cc, 0.05, na.rm = TRUE),
p95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(fig4, aes(time, median_Cc, colour = factor(pump_rpm))) +
geom_hline(yintercept = 1.5, linetype = "dashed", colour = "grey50") +
geom_line() +
facet_grid(dose_mg_h ~ sex_label, scales = "free_y",
labeller = labeller(dose_mg_h = function(x) paste0(x, " mg/h"))) +
scale_colour_brewer("Pump speed (RPM)", palette = "Set1") +
labs(
x = "Time (h)",
y = "Simulated remifentanil concentration (ng/mL)",
title = "Median simulated Cc by sex x ECMO pump speed x infusion rate",
caption = "Replicates Figure 4 of Yang 2017; dashed line = 1.5 ng/mL sedation target."
) +
theme_bw()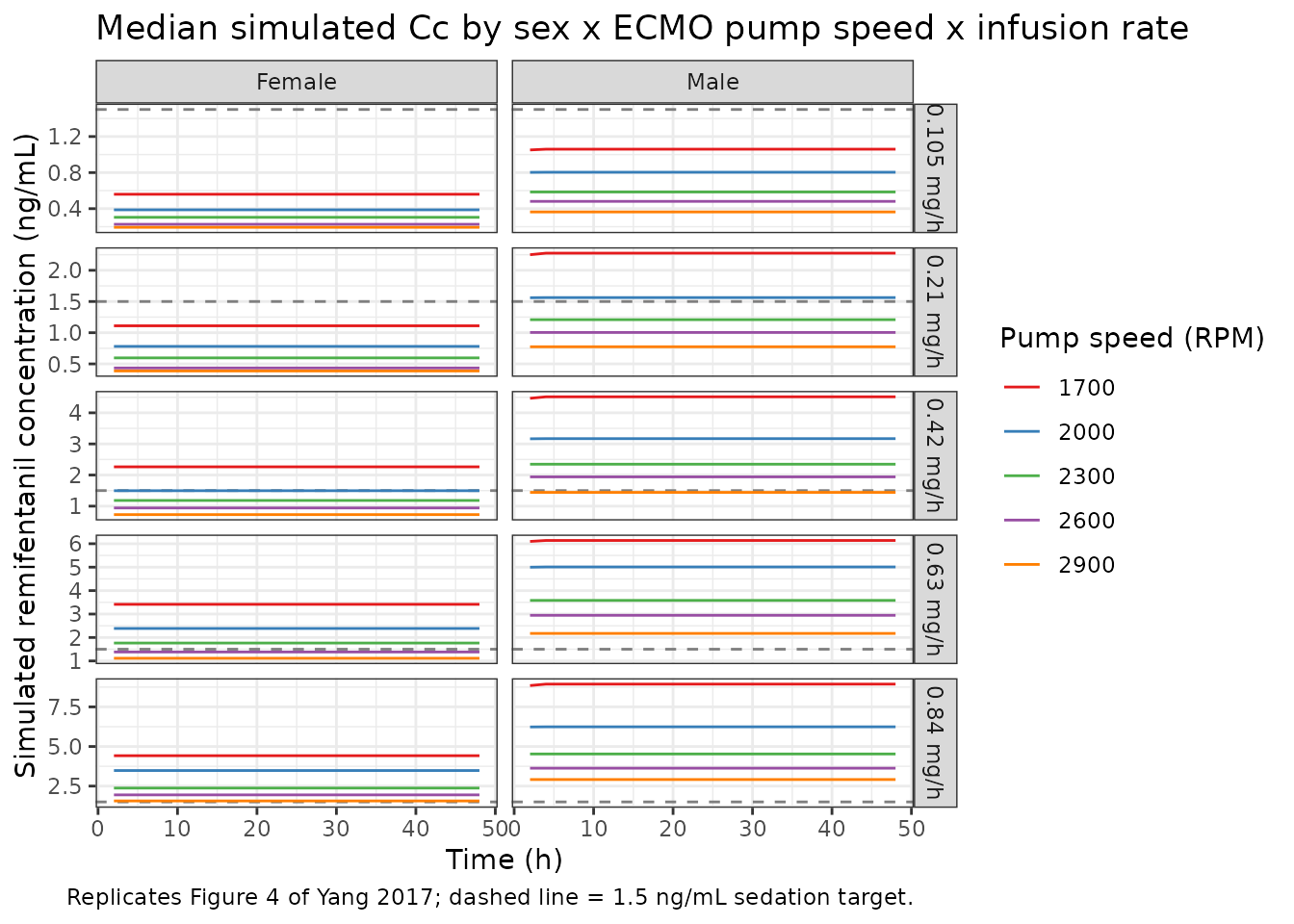
Comparison against the published dosing recommendation
Yang 2017 reports (Results, Predicted concentration profiles):
- For female patients: pump speed 1700-2000 RPM, >= 0.42 mg/h; pump speed 2000-2900 RPM, >= 0.63 mg/h achieves 95% of subjects maintaining Cc >= 1.5 ng/mL.
- For male patients: pump speed 1700-2000 RPM, >= 0.21 mg/h; pump speed 2000-2900 RPM, >= 0.42 mg/h.
Reproduce the same threshold check from the simulated cohort by computing, per (sex, pump speed, dose) cell, the fraction of subjects whose steady-state Cc (taken at t = 48 h) meets or exceeds 1.5 ng/mL.
target_check <- sim |>
dplyr::filter(!is.na(Cc), time == 48) |>
dplyr::group_by(sex_label, pump_rpm, dose_mg_h) |>
dplyr::summarise(
pct_at_target = mean(Cc >= 1.5, na.rm = TRUE) * 100,
median_Cc_48h = median(Cc, na.rm = TRUE),
.groups = "drop"
)
knitr::kable(
target_check |>
dplyr::mutate(
pct_at_target = sprintf("%.0f%%", pct_at_target),
median_Cc_48h = sprintf("%.2f ng/mL", median_Cc_48h)
) |>
tidyr::pivot_wider(
names_from = pump_rpm,
values_from = c(pct_at_target, median_Cc_48h)
),
caption = "Per-cell percentage of virtual subjects at or above 1.5 ng/mL at t = 48 h, and median Cc at t = 48 h. Compare with Yang 2017 dosing recommendation (Results, Predicted concentration profiles)."
)| sex_label | dose_mg_h | pct_at_target_1700 | pct_at_target_2000 | pct_at_target_2300 | pct_at_target_2600 | pct_at_target_2900 | median_Cc_48h_1700 | median_Cc_48h_2000 | median_Cc_48h_2300 | median_Cc_48h_2600 | median_Cc_48h_2900 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Female | 0.105 | 0% | 0% | 0% | 0% | 0% | 0.56 ng/mL | 0.39 ng/mL | 0.30 ng/mL | 0.23 ng/mL | 0.19 ng/mL |
| Female | 0.210 | 0% | 0% | 0% | 0% | 0% | 1.11 ng/mL | 0.78 ng/mL | 0.60 ng/mL | 0.43 ng/mL | 0.39 ng/mL |
| Female | 0.420 | 100% | 48% | 0% | 0% | 0% | 2.26 ng/mL | 1.50 ng/mL | 1.18 ng/mL | 0.94 ng/mL | 0.73 ng/mL |
| Female | 0.630 | 100% | 100% | 88% | 28% | 0% | 3.41 ng/mL | 2.39 ng/mL | 1.76 ng/mL | 1.38 ng/mL | 1.11 ng/mL |
| Female | 0.840 | 100% | 100% | 100% | 96% | 60% | 4.42 ng/mL | 3.48 ng/mL | 2.37 ng/mL | 1.94 ng/mL | 1.56 ng/mL |
| Male | 0.105 | 0% | 0% | 0% | 0% | 0% | 1.06 ng/mL | 0.80 ng/mL | 0.59 ng/mL | 0.48 ng/mL | 0.36 ng/mL |
| Male | 0.210 | 100% | 56% | 4% | 0% | 0% | 2.28 ng/mL | 1.56 ng/mL | 1.21 ng/mL | 1.00 ng/mL | 0.77 ng/mL |
| Male | 0.420 | 100% | 100% | 100% | 96% | 44% | 4.51 ng/mL | 3.17 ng/mL | 2.35 ng/mL | 1.94 ng/mL | 1.44 ng/mL |
| Male | 0.630 | 100% | 100% | 100% | 100% | 100% | 6.14 ng/mL | 5.01 ng/mL | 3.58 ng/mL | 2.95 ng/mL | 2.17 ng/mL |
| Male | 0.840 | 100% | 100% | 100% | 100% | 100% | 8.94 ng/mL | 6.24 ng/mL | 4.53 ng/mL | 3.63 ng/mL | 2.91 ng/mL |
PKNCA validation
PKNCA NCA on the 0-48 h continuous-infusion profile, grouped by sex,
pump speed, and dose. The treatment grouping comes before
id per project convention.
For closed-form sanity-checks at steady state (typical-value, no IIV):
- Steady-state concentration: Css = (infusion rate) / CL_i, where CL_i = 366 x 0.502^SEX x (ECMO_PUMP_SPEED / 2350)^2.04 L/h.
- Elimination half-life: t_(1/2) = ln(2) x V / CL_i. With V = 41 L:
closed_form <- tidyr::expand_grid(
sex_label = names(sexes),
pump_rpm = pump_speeds_rpm,
dose_mg_h = infusion_rates_mg_h
) |>
dplyr::mutate(
sex_male_indicator = ifelse(sex_label == "Male", 1, 0),
CL_Lh = 366 * 0.502^sex_male_indicator * (pump_rpm / 2350)^2.04,
Css_ng_mL = (dose_mg_h * 1000) / CL_Lh,
t_half_min = log(2) * 41 / CL_Lh * 60
)
knitr::kable(
closed_form |>
dplyr::filter(dose_mg_h == 0.35) |>
dplyr::transmute(
Sex = sex_label,
`Pump speed (RPM)` = pump_rpm,
`CL (L/h)` = round(CL_Lh, 1),
`Css at 0.35 mg/h (ng/mL)` = round(Css_ng_mL, 2),
`t_(1/2) (min)` = round(t_half_min, 2)
),
caption = "Closed-form typical-value CL, Css, and t_(1/2) for the cohort-median infusion rate (0.35 mg/h)."
)| Sex | Pump speed (RPM) | CL (L/h) | Css at 0.35 mg/h (ng/mL) | t_(1/2) (min) |
|---|
PKNCA on a manageable subset of the simulation – female / male at the cohort-median pump speed (2300 RPM, nearest grid point to the cohort median of 2350 RPM) and a representative subset of doses:
sim_for_nca <- sim |>
dplyr::filter(pump_rpm == 2300, dose_mg_h %in% c(0.21, 0.42, 0.84), !is.na(Cc)) |>
dplyr::mutate(
treatment = paste0(sex_label, "/", dose_mg_h, "mg/h")
)
sim_nca <- sim_for_nca |>
dplyr::select(id, time, Cc, treatment)
dose_df <- events |>
dplyr::filter(evid == 1, pump_rpm == 2300,
dose_mg_h %in% c(0.21, 0.42, 0.84)) |>
dplyr::transmute(
id = id, time = time, amt = amt,
treatment = paste0(sex_label, "/", dose_mg_h, "mg/h"),
rate = rate, duration = amt / rate
)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id)
dose_obj <- PKNCA::PKNCAdose(
dose_df,
amt ~ time | treatment + id,
duration = "duration"
)
intervals <- data.frame(
start = 0,
end = 48,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE,
cav = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)
knitr::kable(summary(nca_res),
caption = "NCA over the 0-48 h continuous-infusion window for female and male subjects at 2300 RPM and three infusion rates. Cav at steady state equals the closed-form Css = (infusion rate) / CL_i."
)| start | end | treatment | N | auclast | cmax | tmax | cav |
|---|---|---|---|---|---|---|---|
| 0 | 48 | Female/0.21mg/h | 25 | 27.8 [10.2] | 0.591 [10.2] | 6.00 [4.00, 6.00] | 0.579 [10.2] |
| 0 | 48 | Female/0.42mg/h | 25 | 55.5 [11.8] | 1.18 [11.8] | 6.00 [4.00, 6.00] | 1.16 [11.8] |
| 0 | 48 | Female/0.84mg/h | 25 | 110 [11.0] | 2.34 [11.0] | 6.00 [4.00, 6.00] | 2.29 [11.0] |
| 0 | 48 | Male/0.21mg/h | 25 | 57.7 [8.67] | 1.23 [8.67] | 10.0 [8.00, 12.0] | 1.20 [8.67] |
| 0 | 48 | Male/0.42mg/h | 25 | 110 [12.1] | 2.33 [12.1] | 10.0 [8.00, 12.0] | 2.29 [12.1] |
| 0 | 48 | Male/0.84mg/h | 25 | 212 [9.14] | 4.52 [9.14] | 10.0 [8.00, 10.0] | 4.42 [9.14] |
Assumptions and deviations
-
Variance-vs-SD reporting in Table 2. Yang 2017
Methods defines the inter-individual variance as omega^2 and the
residual variance as sigma^2, while Table 2 column headers report
omega CL,sigma proportional, andsigma additivewithout superscripts. The numeric values are interpreted here as the SDs (i.e. the square root of the variances defined in Methods), based on three pieces of evidence: (1) the Greek letter without a^2superscript is the standard mathematical convention for the SD; (2) Table 2 listssigma additive = 0.111 ng/mLin linear concentration units, whereas a variance would carry concentration-squared units (the additive variance interpretation 0.111 (ng/mL)^2 would correspond to SD = 0.333 ng/mL ~= 6.6 x the assay LLOQ of 0.05 ng/mL, larger than expected for a validated LC-MS/MS assay); and (3) this matches the convention used in theAbboud_2009_epinephrinemodel file, whose source paper has an analogous “variance is omega^2, table reports the SD” structure. Theini()block accordingly storesetalcl ~ 0.124^2 = 0.01538(variance, derived from SD = 0.124) and the residual error parameterspropSd = 0.387andaddSd = 0.111 ng/mLas SDs. If a future reading of the original NONMEM control stream shows the Table 2 values were the variances themselves, the encoding would change toetalcl ~ 0.124(variance),propSd = sqrt(0.387) = 0.622, andaddSd = sqrt(0.111) = 0.333 ng/mL. -
Sex encoded under canonical SEXF with an inverted
reference. Yang 2017 uses the male-indicator convention (SEX =
0 female, SEX = 1 male) with female as the structural reference (the
published equation
CL = 366 x 0.502^SEXyields CL = 366 L/h for SEX = 0 / female). To store under the canonical SEXF (1 = female, 0 = male) while preserving the paper’s female-reference CL of 366 L/h, the effect is applied inmodel()asexp(e_sex_cl * (1 - SEXF))withe_sex_cl = log(0.502). This is the same convention asBajaj_2017_nivolumab. - Sex effect should be re-interpreted cautiously. The original paper concludes (Discussion) that “there is no conclusive information indicating that true sex differences exist in the PK of remifentanil due to small sample size and uneven sex ratio in the present study”, with 10 male and 5 female patients in the cohort. The covariate is preserved here because it is part of the published final model, but downstream users should interpret simulated male vs female differences with the same caveat as the paper authors.
- ECMO pump speed as a continuous covariate. Tested as continuous in the source paper (Methods, Covariate model) using power, exponential, and linear forms, with the power form retained. The simulation grid here spans 1700-2900 RPM (Methods, Simulations); extrapolating outside this range is not supported by the source data.
- CRRT tested but not retained. The source paper tested CRRT presence/absence (10/15 patients on CRRT during ECMO support) as a covariate and did not retain it in the final model. The library model therefore does not include RRT_CRRT_STATUS as an effect; the population metadata records the cohort CRRT prevalence (67%) for reference.
-
No bolus dosing. The source cohort received
remifentanil exclusively by continuous infusion (Methods, Study
procedures: “no patients required the bolus injection of remifentanil
during the study”). The library model has no depot / first-order
absorption compartment; the event table dosing convention is to drive
the central compartment with
evid = 1,amt = rate x duration, andrate > 0. -
No IIV on V. The source paper estimated IIV on V as
near zero due to the narrow weight range in the 15-patient cohort
(Results, Population PK analysis), so the final model retains IIV only
on CL. The library model follows the same convention;
vc <- exp(lvc)has no associated eta. -
Pump speed treated as time-fixed. Yang 2017 reports
a per- patient ECMO pump speed (the median over the PK sampling window)
and does not resolve session-level pump-speed changes. The simulation
event table accordingly carries
ECMO_PUMP_SPEEDas a per-subject covariate. For prospective designs that resolve session-level pump-speed adjustments, the covariate is naturally time-varying and the event table would carry one row per time point.