Model and source
- Citation: Ji XW, Ji SM, He XR, Zhu X, Chen R, Lu W. Influences of renal function descriptors on population pharmacokinetic modeling of vancomycin in Chinese adult patients. Acta Pharmacol Sin. 2018;39(2):286-293. doi:10.1038/aps.2017.57 (published online 24 Aug 2017)
- Description: One-compartment IV (intermittent-infusion) population PK model for vancomycin in Chinese adult patients (Ji 2017). Clearance is scaled by raw Cockcroft-Gault creatinine clearance (centered linear term, reference 80 mL/min) and by age (power of (75/age), reference 75 years); the volume of distribution is a single typical value. Developed from steady-state trough therapeutic-drug-monitoring data.
- Article: Acta Pharmacol Sin 2018;39(2):286-293
The article was published online on 24 Aug 2017 (DOI
aps.2017.57) and appeared in the 2018 print volume; the
model file uses the online/DOI year (2017) in its name while the
reference field carries the full 2018 print citation.
Population
The model was developed from routine therapeutic-drug-monitoring data
on 160 hospitalized Chinese adults treated with intravenous vancomycin
(1000 mg every 12 h) at Beijing Hospital, Beijing, China (Ji 2017 Table
1); a further 58 patients were held out for external validation (218
patients in total). None were on renal replacement therapy. Median age
was 78 years (range 42-95), median body weight 65 kg (range 38-90), and
median Cockcroft-Gault creatinine clearance 58.02 mL/min (range
5.45-224.0). 54 of 160 model-building subjects (33.75%) were female. The
dataset contained 251 trough (Cmin) serum vancomycin concentrations
sampled before the next dose; each patient contributed at least one
sample (median 2, range 1-17). Concentrations were measured by TDx-FLx
fluorescence polarization immunoassay (LOQ 2.0 mg/L) and parameters
estimated in NONMEM 7 with FOCEI. The same information is available
programmatically via
readModelDb("Ji_2017_vancomycin")$population.
Source trace
Every numeric value in ini() carries an in-file comment
pointing to the Ji 2017 source location. The table below collects them
in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
lcl (CL) |
2.829 L/h | Eq 16 / Table 3, row “CL (L/h)” (final model) |
lvc (V) |
52.14 L | Eq 17 / Table 3, row “V (L)” (final model) |
e_crcl_cl (theta_CLcr) |
0.00842 | Eq 16 / Table 3, row “theta Clcr_CL” |
e_age_cl (theta_Age) |
0.08143 | Eq 16 + Abstract + Results text |
etalcl (var 0.1051) |
0.1051 | Results text (“variances of 0.1051 and 0.083”) |
etalvc (var 0.083) |
0.083 | Results text (“variances of 0.1051 and 0.083”) |
propSd (26.79% CV) |
0.2679 | Table 3, row “CV (%)” (final model) |
addSd |
2.647 mg/L | Table 3, row “Residual variability SD” (final) |
| CL covariate equation | n/a | Eq 16 |
| Combined residual model | n/a | Eq 2 |
| Exponential IIV model | n/a | Eq 1 |
| CRCL reference (80) | 80 mL/min | Eq 16 / Results text |
| AGE reference (75) | 75 years | Eq 16 / Results text |
| 1-cmt IV structural | n/a | Results para 1; Table 3 (only CL, V estimated) |
The full clearance covariate model (Ji 2017 Eq 16) is
CL = 2.829 * (1 + 0.00842 * (CLcr - 80)) * (75 / Age)^0.08143 * exp(eta1) (L/h)and the volume of distribution (Eq 17) is
V = 52.14 * exp(eta2) (L).
Virtual cohort
Original observed data are not publicly available. The cohort below covers four scenarios bracketing the paper’s covariate space: the typical model-building subject (median age, median CRCL), a good-renal-function subject, a poor-renal-function subject, and a younger high-clearance subject. All receive the studied regimen of 1000 mg every 12 h as a 1-hour IV infusion, simulated to steady state.
set.seed(20260527)
n_sub <- 120L
tau <- 12 # dosing interval (h)
n_dose <- 14L # number of q12h doses -> steady state
dose_times <- seq(0, by = tau, length.out = n_dose)
last_dose <- max(dose_times) # 156 h
ss_end <- last_dose + tau # 168 h
# Observation grid: coarse over the whole horizon for the VPC, dense over the
# final (steady-state) dosing interval for NCA.
obs_times <- sort(unique(c(
seq(0, ss_end, by = 3),
seq(last_dose, ss_end, by = 0.5)
)))
build_arm <- function(label, age, crcl, id_offset) {
ids <- id_offset + seq_len(n_sub)
dose_rows <- tidyr::expand_grid(id = ids, time = dose_times) |>
mutate(
evid = 1L,
amt = 1000,
cmt = "central",
rate = 1000 / 1, # 1000 mg infused over 1 hour
cohort = label,
AGE = age,
CRCL = crcl
)
obs_rows <- tidyr::expand_grid(id = ids, time = obs_times) |>
mutate(
evid = 0L,
amt = 0,
cmt = NA_character_,
rate = 0,
cohort = label,
AGE = age,
CRCL = crcl
)
bind_rows(dose_rows, obs_rows) |> arrange(id, time, desc(evid))
}
events <- bind_rows(
build_arm("age78_crcl58", 78, 58, 0L), # typical model-building subject
build_arm("age78_crcl120", 78, 120, 120L), # good renal function
build_arm("age78_crcl20", 78, 20, 240L), # poor renal function
build_arm("age50_crcl120", 50, 120, 360L) # younger, high clearance
)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Ji_2017_vancomycin")
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("cohort", "AGE", "CRCL")
) |> as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'For the typical-value reproduction of Eq 16 (no between-subject variability), also simulate with the random effects zeroed:
mod_typical <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
sim_typical <- rxode2::rxSolve(
mod_typical,
events = events,
keep = c("cohort", "AGE", "CRCL")
) |> as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc'
#> Warning: multi-subject simulation without without 'omega'Replicate published figures
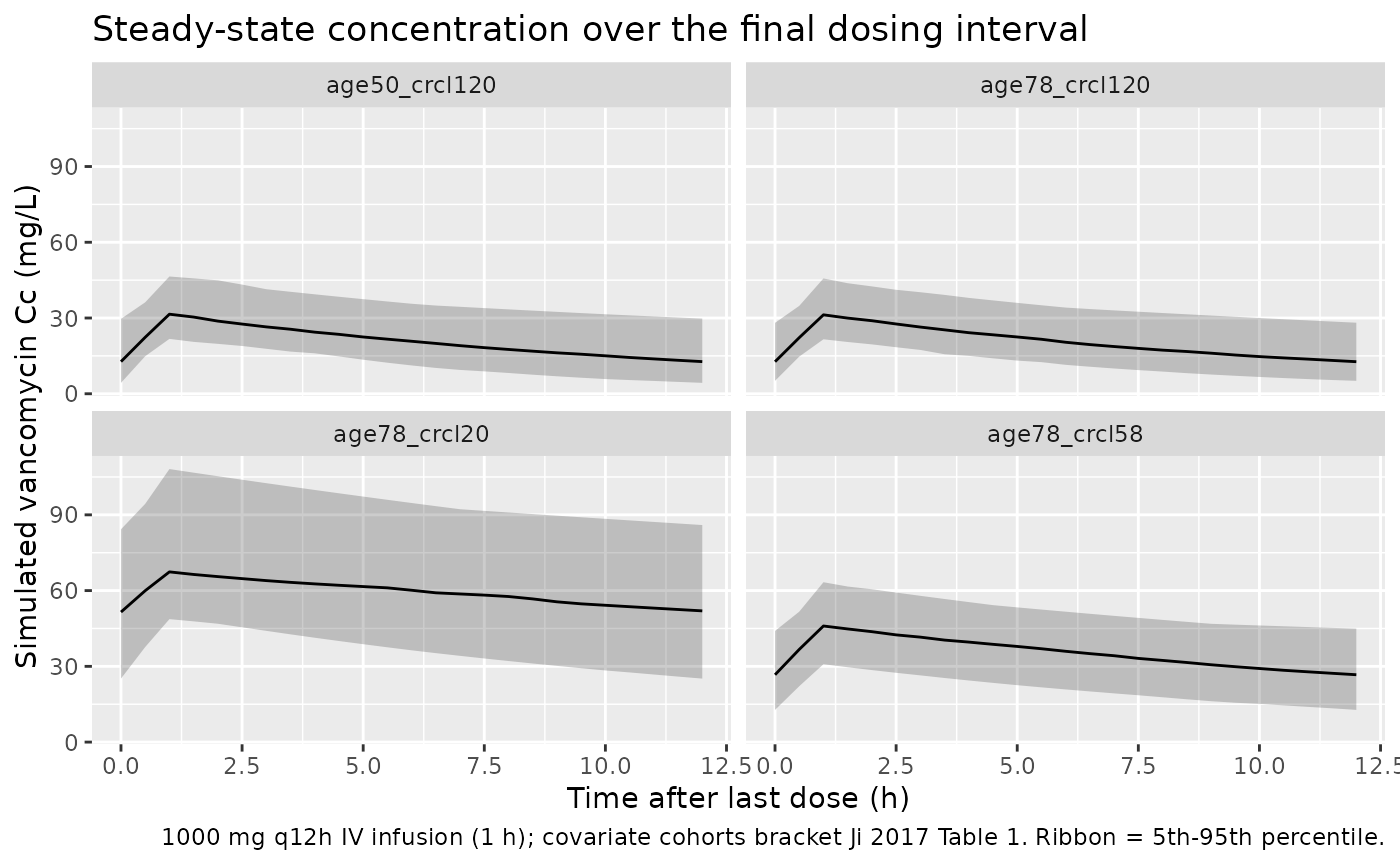
Ji 2017 Figure 2 is a visual predictive check of trough concentrations and Figure 1 shows observed-vs-predicted goodness-of-fit clouds; neither is a per-subject concentration-time curve that can be reproduced directly. The block below summarises the simulated steady-state concentration-time profile for each covariate cohort, illustrating the renal- and age-dependent accumulation that drives the paper’s dose-individualisation analysis.
sim |>
filter(time >= last_dose) |>
mutate(tad = time - last_dose) |>
group_by(cohort, tad) |>
summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot(aes(tad, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
geom_line() +
facet_wrap(~ cohort) +
labs(
x = "Time after last dose (h)",
y = "Simulated vancomycin Cc (mg/L)",
title = "Steady-state concentration over the final dosing interval",
caption = "1000 mg q12h IV infusion (1 h); covariate cohorts bracket Ji 2017 Table 1. Ribbon = 5th-95th percentile."
)
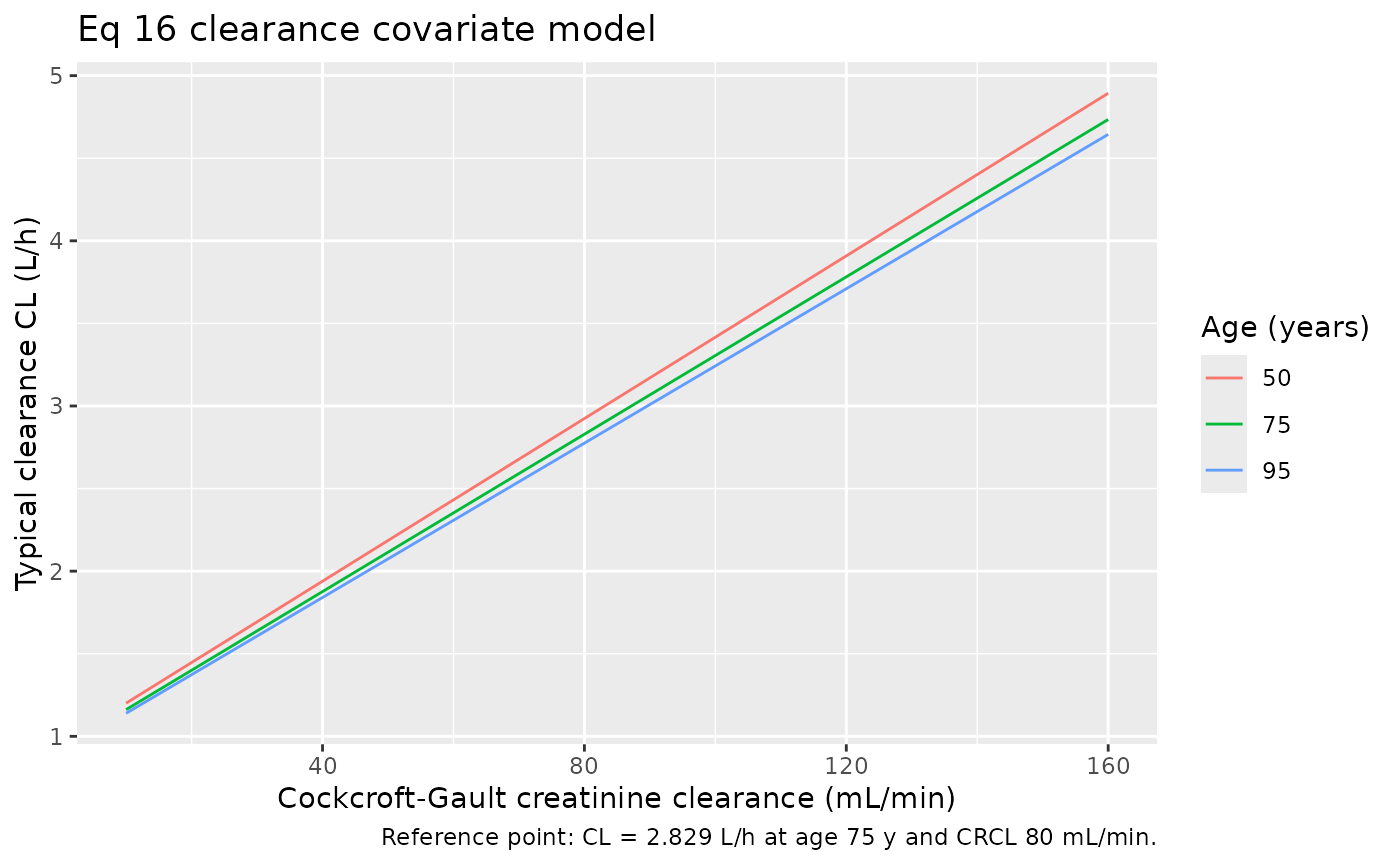
The clearance covariate relationships of Eq 16 (CL rises with creatinine clearance and falls with age) are reproduced directly from the packaged model’s typical-value clearance:
cov_grid <- tidyr::expand_grid(
AGE = c(50, 75, 95),
CRCL = seq(10, 160, by = 10)
) |>
mutate(CL = 2.829 * (1 + 0.00842 * (CRCL - 80)) * (75 / AGE)^0.08143)
ggplot(cov_grid, aes(CRCL, CL, colour = factor(AGE))) +
geom_line() +
labs(
x = "Cockcroft-Gault creatinine clearance (mL/min)",
y = "Typical clearance CL (L/h)",
colour = "Age (years)",
title = "Eq 16 clearance covariate model",
caption = "Reference point: CL = 2.829 L/h at age 75 y and CRCL 80 mL/min."
)
PKNCA validation
Ji 2017 does not publish an NCA table (Cmax / AUC); the model was
built on trough concentrations and used to drive a dose-targeting
simulation. The PKNCA block below characterises the steady-state
interval metrics (Cmax,ss, Tmax, Cmin/Ctrough = trough, Cavg, AUC0-tau)
over the final dosing interval for each covariate cohort, providing a
one-table audit of the simulated steady-state exposure. The treatment
grouping is cohort.
sim_nca <- sim |>
filter(!is.na(Cc), time >= last_dose) |>
select(id, time, Cc, cohort)
dose_df <- events |>
filter(evid == 1, time == last_dose) |>
select(id, time, amt, cohort)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | cohort + id,
concu = "mg/L", timeu = "hr")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | cohort + id,
doseu = "mg")
intervals <- data.frame(
start = last_dose,
end = ss_end,
cmax = TRUE,
tmax = TRUE,
cmin = TRUE,
ctrough = TRUE,
cav = TRUE,
auclast = TRUE
)
nca_res <- PKNCA::pk.nca(
PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
)
nca_summary <- summary(nca_res)
knitr::kable(
nca_summary,
caption = "Simulated steady-state NCA parameters by covariate cohort (1000 mg q12h IV infusion, final dosing interval)."
)| Interval Start | Interval End | cohort | N | AUClast (hr*mg/L) | Cmax (mg/L) | Cmin (mg/L) | Tmax (hr) | Cav (mg/L) | Ctrough (mg/L) |
|---|---|---|---|---|---|---|---|---|---|
| 156 | 168 | age50_crcl120 | 120 | 247 [34.2] | 31.5 [24.0] | 12.1 [58.4] | 1.00 [1.00, 1.00] | 20.6 [34.2] | NC |
| 156 | 168 | age78_crcl120 | 120 | 248 [35.3] | 31.8 [24.4] | 11.9 [65.0] | 1.00 [1.00, 1.00] | 20.6 [35.3] | NC |
| 156 | 168 | age78_crcl20 | 120 | 709 [32.3] | 69.0 [27.3] | 49.7 [39.1] | 1.00 [1.00, 1.00] | 59.1 [32.3] | NC |
| 156 | 168 | age78_crcl58 | 120 | 417 [29.8] | 45.0 [23.8] | 25.8 [40.8] | 1.00 [1.00, 1.00] | 34.7 [29.8] | NC |
Comparison against published values
Ji 2017 reports no Cmax / AUC NCA table, so there is no published NCA row to compare against directly. The two checks below validate that the packaged model reproduces the paper’s structural parameter relationships.
# Typical clearance at the published reference point and at illustrative
# covariate values, computed (a) by hand from Eq 16 and (b) from the
# zero-random-effect simulation.
ref_check <- sim_typical |>
# sim_typical retains per-subject cl/vc values inherited from the
# preceding `sim` simulation's IIV state, so unique(cl) can return >1
# value within a cohort. mean() collapses the per-id values back to
# the typical-value cohort summary that this table is meant to show.
group_by(cohort, AGE, CRCL) |>
summarise(CL_model = mean(cl), V_model = mean(vc), .groups = "drop") |>
mutate(
CL_eq16 = 2.829 * (1 + 0.00842 * (CRCL - 80)) * (75 / AGE)^0.08143,
V_eq17 = 52.14
) |>
select(cohort, AGE, CRCL, CL_eq16, CL_model, V_eq17, V_model)
knitr::kable(
ref_check,
caption = "Typical CL (Eq 16) and V (Eq 17): hand-computed vs packaged-model values.",
digits = 3
)| cohort | AGE | CRCL | CL_eq16 | CL_model | V_eq17 | V_model |
|---|---|---|---|---|---|---|
| age50_crcl120 | 50 | 120 | 3.909 | 3.909 | 52.14 | 52.14 |
| age78_crcl120 | 78 | 120 | 3.770 | 3.770 | 52.14 | 52.14 |
| age78_crcl20 | 78 | 20 | 1.395 | 1.395 | 52.14 | 52.14 |
| age78_crcl58 | 78 | 58 | 2.298 | 2.298 | 52.14 | 52.14 |
The packaged model returns CL = 2.829 L/h and V = 52.14 L at the reference subject (age 75 y, CRCL 80 mL/min), matching Ji 2017 Eq 16-17 / Table 3 exactly, and reproduces the hand-computed Eq 16 clearance at every cohort. Across the renal-function range the simulated steady-state troughs span roughly 14 mg/L (high clearance) to ~50 mg/L (CRCL 20 mL/min) for a fixed 1000 mg q12h regimen, consistent with the paper’s finding that renal function dominates vancomycin exposure and that dose individualisation is required to keep troughs within the 10-15 / 15-20 mg/L targets.
Assumptions and deviations
-
Age covariate coefficient (0.08143, not 0.8143). Ji
2017 Eq 16, the Abstract, and the Results text all state the age
exponent as 0.08143. Table 3 prints
theta Age_CL = 0.8143(RSE 53.68%) with bootstrap median0.8373– a 10x discrepancy. The packaged model uses 0.08143 because three independent statements (the model-defining equation, the abstract, and the Results narrative) agree on it, and only the single Table 3 cell (plus its bootstrap row) carries the larger value, which is a dropped-leading-zero typographical error. The directionality is also a cross-check: the paper states vancomycin excretion decreases as renal function diminishes with age, which(75/Age)^0.08143reproduces (CL falls as age rises above 75). Europe PMC (PMID 28836582) lists no erratum or corrigendum for this article. - Additive residual error units (mg/L, not ng/mL). Table 3 labels the additive residual row “Residual variability SD (ng/mL)” = 2.647, but the vancomycin concentration unit is mg/L throughout the paper (Table 1, LOQ 2.0 mg/L, target troughs in mg/L). An additive SD of 2.647 ng/mL (= 0.0026 mg/L) would be negligible and incompatible with the authors’ choice of a combined error model, whereas 2.647 mg/L is a sensible additive term near the 2.0 mg/L LOQ. The packaged model therefore treats 2.647 as mg/L; the “(ng/mL)” column label is read as a units typo.
-
One-compartment IV, no absorption compartment. The
Abstract and Results describe “first-order absorption” while the
Discussion says “zero-order absorption”, but vancomycin was given by
intravenous infusion and Table 3 estimates only CL and V (no absorption
rate constant). The drug is therefore dosed directly into the central
compartment as an IV infusion; no depot /
kais included, since none was estimated and inventing one is not supported by the source. -
IIV variances taken from the Results text. The
Results state the eta variances directly (“variances of 0.1051 and
0.083, respectively”) for CL and V; these go into
ini()as the omega values (etalcl ~ 0.1051,etalvc ~ 0.083). They reproduce the Table 3 “IIV (%)” rows on the square-root scale (sqrt(0.1051) = 32.4%; sqrt(0.083) = 28.8%). - Infusion duration. The paper records “continuous infusion of vancomycin (1000 mg q12 h)” with trough sampling before the next dose, i.e. intermittent q12h infusions. The infusion duration is not stated; the vignette assumes a 1-hour infusion (a common vancomycin practice and the same convention used in the Goti 2018 vancomycin vignette). The infusion duration has negligible effect on the modeled trough concentrations.
-
Year in the file name. The article was published
online in 2017 (DOI
10.1038/aps.2017.57) and in print in 2018 (Acta Pharmacol Sin 39(2):286-293). The model file / vignette name uses 2017 (online/DOI year); thereferencefield gives the full 2018 print citation. - Dose-individualisation supplements not used. The dosing-regimen tables (Tables S1-S4) referenced for the 10-15 and 15-20 mg/L trough targets are simulation outputs in the journal’s supplementary information and were not available on disk. They contain no model parameters (all final estimates are in Eq 16-17 and Table 3), so their absence does not affect the packaged model.
- Virtual-cohort demographics. Race / ethnicity beyond “Chinese adults” is not reported and is not a model covariate; the virtual cohort fixes age and CRCL per arm to illustrate the covariate effects rather than sampling the full joint demographic distribution.