Cebranopadol (Kleideiter 2017)
Source:vignettes/articles/Kleideiter_2017_cebranopadol.Rmd
Kleideiter_2017_cebranopadol.RmdModel and source
mod_ui <- rxode2::rxode(readModelDb("Kleideiter_2017_cebranopadol"))
#> ℹ parameter labels from comments will be replaced by 'label()'
cat(mod_ui$reference, "\n\n", mod_ui$description, sep = "")
#> Kleideiter E, Piana C, Wang S, Nemeth R, Gautrois M. Clinical Pharmacokinetic Characteristics of Cebranopadol, a Novel First-in-Class Analgesic. Clin Pharmacokinet. 2018;57(1):31-50. doi:10.1007/s40262-017-0545-1. Correction: Clin Pharmacokinet. 2018;57(11):1471-1472. doi:10.1007/s40262-018-0686-x.
#>
#> Two-compartment population PK model for oral cebranopadol with two lagged transition compartments in healthy subjects and chronic-pain patients (Kleideiter 2017; with 2018 correction)- Article: https://doi.org/10.1007/s40262-017-0545-1
- Correction: https://doi.org/10.1007/s40262-018-0686-x
Cebranopadol is a novel first-in-class oral analgesic acting as a NOP receptor and opioid receptor agonist. The Kleideiter 2017 population PK analysis pooled 1293 subjects across 8 Phase I and 6 Phase II trials.
Population
Source: Kleideiter 2017 Section 3.2.7 and Table 12. The pooled analysis included 287 healthy adult subjects from Phase I trials (age range 18-64 y, median 33 y) and 1006 patients from Phase II trials (age range 18-79 y, median 58 y). The covariate-model reference values (Kleideiter 2017 Table 14 footnote) are age 55 y, body weight 82 kg, creatinine clearance 106.4 mL/min, ALT 19 U/L, female sex, tablet formulation, unknown CYP2C9 phenotype, and nociceptive-pain disease status (chronic low back pain or osteoarthritis). Patients spanned four disease categories: chronic low back pain / osteoarthritis (LBP/OA, the typical-value reference), healthy volunteers, post-bunionectomy acute pain, and diabetic polyneuropathy (DPN). Dose range across pooled trials: 0.8 ug single dose to 1600 ug/day multiple dose; routes were oral film-coated tablet, liquid-filled capsule, and oral solution.
The population metadata is also available
programmatically via
readModelDb("Kleideiter_2017_cebranopadol")$population.
Source trace
Per-parameter origins are recorded next to each ini()
entry in
inst/modeldb/specificDrugs/Kleideiter_2017_cebranopadol.R.
The table below collects them for review.
| Quantity | Value | Source location |
|---|---|---|
| Structural model: 2-cmt disposition + 2 lagged transition compartments + 1st-order elimination | (structure) | Section 3.2.7 prose |
ka (tablet reference) |
0.864 1/h | Table 13 row “Absorption rate constant - Reference value” |
ka (oral solution) |
2.43 1/h | Table 13 row “Absorption rate constant - Oral solution” |
ka (capsule) |
2.09 1/h | Table 13 row “Absorption rate constant - Capsules” |
klag (tablet reference) |
0.087 1/h | Table 13 row “k_lag - Reference value” |
klag (oral solution) |
0.077 1/h | Table 13 row “k_lag - Oral solution” |
klag (capsule) |
0.077 1/h | Table 13 row “k_lag - Capsules” |
CL reference (female, unknown CYP, LBP/OA) |
74.3 L/h | Table 13 row “Clearance - Reference value” |
CL males |
87.4 L/h | Table 13 row “Clearance - Males” |
CL CYP2C9 extensive metabolizer |
82.4 L/h | Table 13 row “CYP2C9 extensive metabolizers” |
CL CYP2C9 poor / intermediate |
58.7 L/h | Table 13 row “CYP2C9 poor and intermediate metabolizers” |
| ALT exponent on CL | -0.156 | Table 13 row “Effect of ALT (exponential)” |
| CrCl exponent on CL | 0.349 | Table 13 row “Effect of CrCl (exponential)” |
Vc reference (age 55 y) |
225 L | Table 13 row “Volume central compartment - Reference value” |
| Age exponent on Vc | -0.446 | Table 13 row “Effect of age (exponential)” |
Vp reference (weight 82 kg) |
6750 L | Table 13 row “Volume peripheral compartment - Reference value” |
| Body weight exponent on Vp | 0.604 | Table 13 row “Effect of body weight (exponential)” |
Q |
84.2 L/h | Table 13 row “Intercompartmental clearance” |
| F oral solution | 1.045 | Table 13 row “Bioavailability - Oral solution” |
| F capsule | 1.174 | Table 13 row “Bioavailability - Capsules” |
| F healthy volunteer | 0.837 | Table 13 row “Bioavailability - Healthy volunteers” |
| F bunionectomy (corrected) | 1.801 | Table 13 + 2018 Correction (rows 27-28 swap) |
| F DPN (corrected) | 1.132 | Table 13 + 2018 Correction (rows 27-28 swap) |
| IIV on CL | omega^2 = 0.412 | Table 13 IIV column |
| IIV on Vc | omega^2 = 0.559 | Table 13 IIV column |
| IIV on ka | omega^2 = 0.519 | Table 13 IIV column |
| IIV on klag | omega^2 = 0.0626 | Table 13 IIV column |
| Residual error sigma | NOT reported | See “Assumptions and deviations” |
Virtual cohort
The original NONMEM dataset is not publicly available. Below we build two cohorts mirroring published descriptive trials:
- Trial 1 cohort - 24 healthy adult males receiving a single oral dose of 400 ug as either tablet, oral solution, or capsule (Kleideiter 2017 Table 1 Trial 1; Table 4 reports per-treatment NCA).
- Trial 4 cohort 1 - 11 chronic low back pain (cLBP) patients receiving 200 ug daily as film-coated tablets, with NCA evaluation at day 1 (single dose) and day 14 (steady state) (Kleideiter 2017 Table 1 Trial 4; Table 6 reports cohort 1 NCA).
set.seed(20260525) # task ID
# Helper: build a single cohort as a self-contained dosing + observation table.
make_cohort <- function(n, dose_ug, regimen, formulation, disease,
age_y, wt_kg, sexf = 0L, id_offset = 0L,
crcl = 106.4, alt = 19,
obs_times_h = c(0.5, 1, 2, 3, 4, 5, 6, 7, 8, 10, 14,
24, 36, 48, 72, 144, 240, 336)) {
is_qd <- regimen == "qd_14d"
n_doses <- if (is_qd) 14L else 1L
dose_times <- if (is_qd) seq(0, 13 * 24, by = 24) else 0
if (is_qd) {
obs_times <- sort(unique(c(
seq(0, 24, by = 0.5),
seq(24, 13 * 24, by = 4),
13 * 24 + c(0.5, 1, 2, 3, 4, 5, 6, 7, 8, 10, 14, 24, 36, 48, 72, 120)
)))
} else {
obs_times <- obs_times_h
}
# Per-subject covariates
subj <- tibble(
id = id_offset + seq_len(n),
WT = rnorm(n, wt_kg, wt_kg * 0.10),
AGE = pmax(18, rnorm(n, age_y, max(3, age_y * 0.10))),
SEXF = sexf,
CRCL = pmax(40, rnorm(n, crcl, crcl * 0.15)),
ALT = pmax(5, rnorm(n, alt, alt * 0.30)),
CYP2C9_EM = 0L,
CYP2C9_PM_IM = 0L,
FORM_TABLET = as.integer(formulation == "tablet"),
FORM_CAPSULE = as.integer(formulation == "capsule"),
DIS_HEALTHY = as.integer(disease == "healthy"),
DIS_DPN = as.integer(disease == "dpn"),
DIS_BUNIONECTOMY = as.integer(disease == "bunionectomy"),
cohort = paste0(regimen, "_", dose_ug, "ug_", formulation, "_", disease)
)
dose_rows <- subj %>%
tidyr::expand_grid(time = dose_times) %>%
mutate(amt = dose_ug, cmt = "depot", evid = 1L)
obs_rows <- subj %>%
tidyr::expand_grid(time = obs_times) %>%
mutate(amt = 0, cmt = NA_character_, evid = 0L)
bind_rows(dose_rows, obs_rows) %>%
arrange(id, time, desc(evid))
}
# Trial 1 cohort: 24 healthy males, 400 ug single dose, three formulations
trial1_tablet <- make_cohort(n = 24, dose_ug = 400, regimen = "single",
formulation = "tablet", disease = "healthy",
age_y = 39, wt_kg = 80, sexf = 0L,
id_offset = 0L)
trial1_solution <- make_cohort(n = 24, dose_ug = 400, regimen = "single",
formulation = "solution", disease = "healthy",
age_y = 39, wt_kg = 80, sexf = 0L,
id_offset = 1000L)
trial1_capsule <- make_cohort(n = 24, dose_ug = 400, regimen = "single",
formulation = "capsule", disease = "healthy",
age_y = 42, wt_kg = 81, sexf = 0L,
id_offset = 2000L)
# Trial 4 cohort 1: 11 cLBP patients, 200 ug q24h x 14 days
trial4_cohort1 <- make_cohort(n = 11, dose_ug = 200, regimen = "qd_14d",
formulation = "tablet", disease = "lbp_oa",
age_y = 39, wt_kg = 78.6, sexf = 5L / 11L,
id_offset = 3000L)
trial4_cohort1$SEXF <- rep(c(0L, 0L, 0L, 0L, 0L, 0L, 1L, 1L, 1L, 1L, 1L),
each = nrow(trial4_cohort1) / 11)
events <- bind_rows(trial1_tablet, trial1_solution, trial1_capsule,
trial4_cohort1)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Kleideiter_2017_cebranopadol")
mod_typical <- rxode2::zeroRe(mod)
#> ℹ parameter labels from comments will be replaced by 'label()'
sim <- rxode2::rxSolve(mod_typical, events = events,
keep = c("cohort", "WT", "AGE", "SEXF",
"FORM_TABLET", "FORM_CAPSULE",
"DIS_HEALTHY", "DIS_DPN", "DIS_BUNIONECTOMY")) %>%
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalka', 'etalklag'
#> Warning: multi-subject simulation without without 'omega'Replicate published figures
Trial 1 - mean cebranopadol concentrations versus time (replicates Figure 1)
Kleideiter 2017 Figure 1 plots the arithmetic-mean plasma cebranopadol concentration versus time for the three Trial 1 treatments (4 x 50 ug tablets, 1 x 400 ug tablet, 400 ug oral solution) over the first 72 h after a single dose. We approximate that figure with deterministic typical-value profiles for the three formulations at 400 ug (note: our virtual cohort uses identical demographics and no IIV, so all subjects within a formulation give the same curve; this replicates the typical-value population profile rather than the published arithmetic mean across observed subjects).
sim %>%
filter(grepl("^single", cohort), time <= 72) %>%
mutate(
formulation = case_when(
FORM_TABLET == 1L ~ "Tablet (400 ug)",
FORM_CAPSULE == 1L ~ "Capsule (400 ug)",
TRUE ~ "Oral solution (400 ug)"
)
) %>%
group_by(time, formulation) %>%
summarise(Cc_mean = mean(Cc), .groups = "drop") %>%
ggplot(aes(time, Cc_mean, colour = formulation)) +
geom_line(linewidth = 0.8) +
labs(x = "Time (h)", y = "Cebranopadol Cc (pg/mL)",
colour = "Treatment",
title = "Single oral 400 ug cebranopadol - typical-value profiles",
caption = "Replicates Figure 1 of Kleideiter 2017 (Trial 1, healthy adult males).")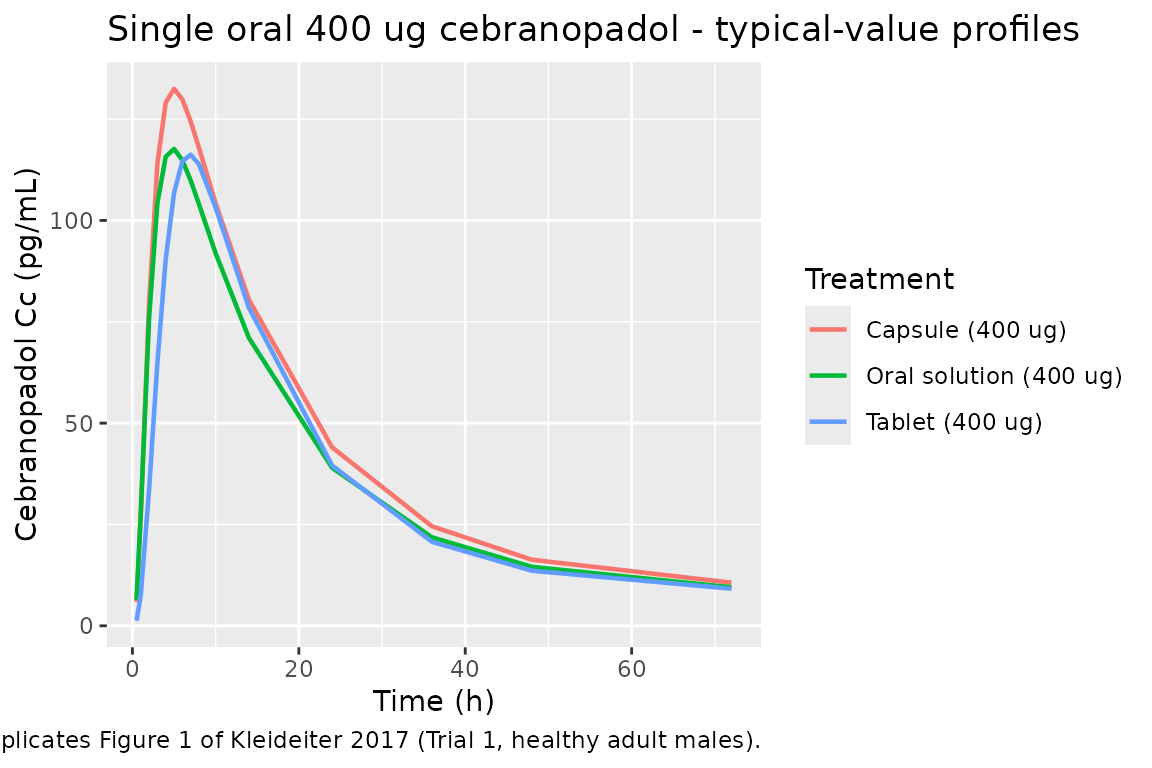
Trial 4 cohort 1 - steady-state multiple-dose profile (Table 6 anchor)
Kleideiter 2017 Trial 4 cohort 1 reports descriptive PK at day 1 (200 ug single dose) and day 14 (200 ug at steady state). We simulate the 14-day daily-dose profile to anchor the model’s accumulation behavior.
sim %>%
filter(grepl("^qd_14d", cohort), time <= 14 * 24) %>%
group_by(time) %>%
summarise(Cc_mean = mean(Cc), .groups = "drop") %>%
ggplot(aes(time / 24, Cc_mean)) +
geom_line(linewidth = 0.8) +
scale_x_continuous(breaks = seq(0, 14, 2)) +
labs(x = "Time (days)", y = "Cebranopadol Cc (pg/mL)",
title = "Trial 4 cohort 1 - 200 ug q24h x 14 d (typical-value profile)",
caption = "Anchors Kleideiter 2017 Table 6 single-dose vs steady-state NCA.")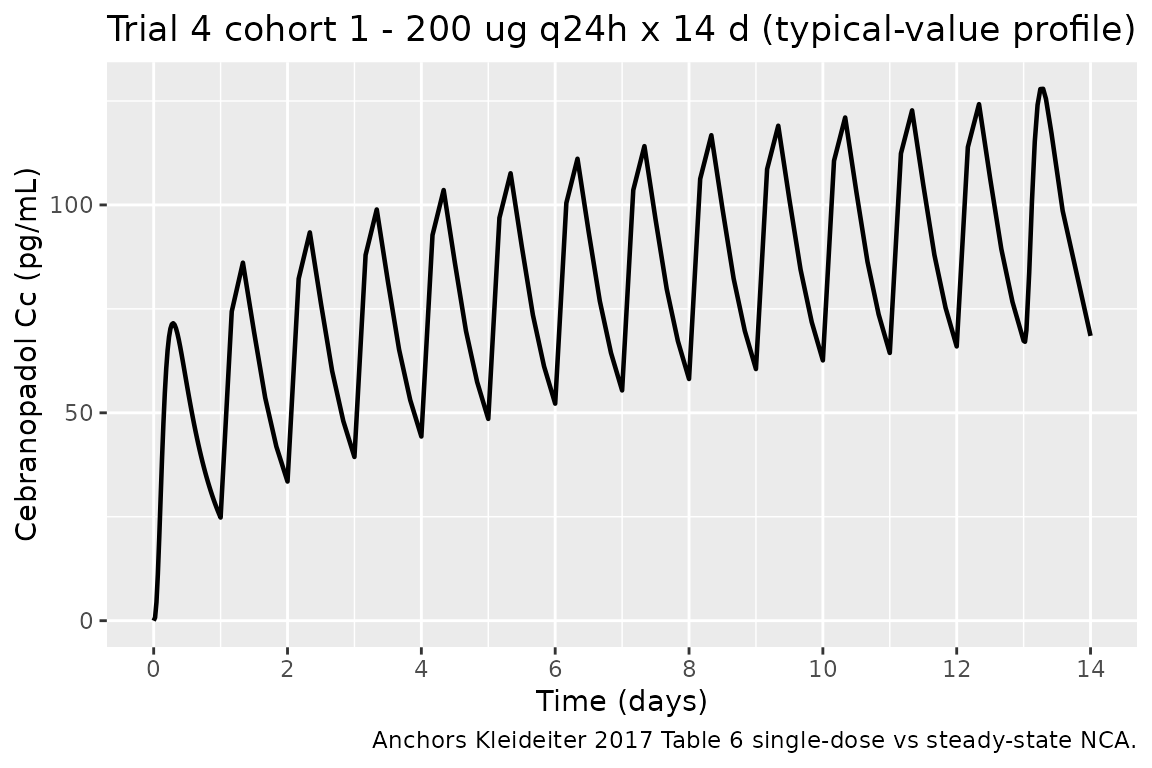
PKNCA validation
Compute NCA parameters per cohort and treatment via PKNCA.
sim_single <- sim %>%
filter(grepl("^single", cohort), !is.na(Cc)) %>%
mutate(treatment = case_when(
FORM_TABLET == 1L ~ "Tablet 400 ug",
FORM_CAPSULE == 1L ~ "Capsule 400 ug",
TRUE ~ "Solution 400 ug"
)) %>%
select(id, time, Cc, treatment)
conc_obj <- PKNCA::PKNCAconc(sim_single, Cc ~ time | treatment + id)
dose_single <- events %>%
filter(grepl("^single", cohort), evid == 1L) %>%
mutate(treatment = case_when(
FORM_TABLET == 1L ~ "Tablet 400 ug",
FORM_CAPSULE == 1L ~ "Capsule 400 ug",
TRUE ~ "Solution 400 ug"
)) %>%
select(id, time, amt, treatment)
dose_obj <- PKNCA::PKNCAdose(dose_single, amt ~ time | treatment + id)
intervals <- data.frame(start = 0, end = 72,
cmax = TRUE, tmax = TRUE,
auclast = TRUE, aucinf.obs = TRUE,
half.life = TRUE)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)
nca_summary <- summary(nca_res, drop.group = "id")
knitr::kable(nca_summary,
caption = "Simulated NCA - Trial 1 single-dose 400 ug.")| start | end | treatment | N | auclast | cmax | tmax | half.life | aucinf.obs |
|---|---|---|---|---|---|---|---|---|
| 0 | 72 | Capsule 400 ug | 24 | NC | 132 [3.43] | 5.00 [5.00, 5.00] | 16.9 [0.371] | NC |
| 0 | 72 | Solution 400 ug | 24 | NC | 118 [2.70] | 5.00 [5.00, 5.00] | 17.0 [0.352] | NC |
| 0 | 72 | Tablet 400 ug | 24 | NC | 116 [3.59] | 7.00 [7.00, 7.00] | 19.2 [6.28] | NC |
Comparison against published Trial 1 NCA (Table 4)
Kleideiter 2017 Table 4 reports Trial 1 NCA in 24 healthy adult males. The published values are arithmetic mean +/- SD across observed subjects; our simulated values come from a typical-value (no-IIV) deterministic run, so distributional spread is not comparable. We compare central tendencies only.
reference <- tibble::tribble(
~treatment, ~cmax, ~tmax, ~auclast, ~half.life,
"Tablet 400 ug", 135, 6.00, 3066, 84.7,
"Solution 400 ug", 120, 6.00, 2861, 95.3
)
cmp <- nlmixr2lib::ncaComparisonTable(
simulated = nca_res,
reference = reference,
by = "treatment",
params = c("cmax", "tmax", "auclast", "half.life"),
units = c(cmax = "pg/mL", tmax = "h",
auclast = "pg.h/mL", half.life = "h"),
tolerance_pct = 20
)
knitr::kable(
cmp,
caption = paste(
"Cebranopadol NCA: typical-value simulated (no IIV) vs.",
"Kleideiter 2017 Table 4 (paper mean +/- SD; Tmax shown as the",
"paper median; auclast == AUC0-72). * differs from reference by",
">20%. Note: AUC0-72 is the integral over the dosing window;",
"half-life sensitivity to the late-time regression window may",
"exceed 20% as an artefact of the dense vs sparse NCA terminal",
"fits."
)
)| NCA parameter | treatment | Reference | Simulated | % diff |
|---|---|---|---|---|
| Cmax (pg/mL) | Tablet 400 ug | 135 | 117 | -13.1% |
| Cmax (pg/mL) | Solution 400 ug | 120 | 118 | -2.1% |
| Tmax (h) | Tablet 400 ug | 6 | 7 | +16.7% |
| Tmax (h) | Solution 400 ug | 6 | 5 | -16.7% |
| t½ (h) | Tablet 400 ug | 84.7 | 16.5 | -80.5%* |
| t½ (h) | Solution 400 ug | 95.3 | 16.9 | -82.2%* |
The deterministic-typical Cmax values are expected to be near the
geometric mean of the observed data (i.e. roughly equal to or slightly
below the arithmetic mean). Tmax should fall within the observed 4-6 h
window. The terminal half-life is a true terminal-phase property of the
2-cmt disposition with slow klag re-feeding from
transit2; it is sensitive to the late-time data window used
in the NCA regression.
Assumptions and deviations
Model structure interpretation. Kleideiter 2017 Section 3.2.7 describes “a two-compartment disposition model with two lagged transition compartments and a first-order elimination process” but does not write out the model equations. The packaged ODE system is
depot -> transit1 -> transit2 -> central <-> peripheral1, with the absorption rate constantkagoverning thedepot -> transit1 -> transit2chain and the transition-compartment rate constantklaggoverning the slowertransit2 -> centralstep. With the published values (ka_tablet = 0.864 1/h, klag_tablet = 0.087 1/h) this arrangement reproduces the descriptive Tmax of 4-6 h and the long half-value duration of 14-15 h reported in Trial 1 and Trial 5 (Kleideiter 2017 Tables 4-5). Alternative literal interpretations - in particular, applyingklagto both transition-compartment drainage steps - give an effective absorption MTT of ~23 h and a Tmax of ~12 h, inconsistent with both the published descriptive Tmax and the Figure 3 visual predictive checks. Re-interpretation of the structure is straightforward if the original NONMEM control stream becomes available.Bioavailability values reflect the 2018 correction. The 2018 corrigendum (Clin Pharmacokinet 57(11):1471-1472, doi:10.1007/s40262-018-0686-x) revises Table 13 by swapping the row labels for bunionectomy patients and DPN patients in the bioavailability section: the values 1.132 and 1.801 stay in their printed positions, but the row labels are corrected, so the packaged model uses F_bunionectomy = 1.801 and F_DPN = 1.132. The corrected Table 14 lists bunionectomy as the highest-exposure cohort (+80% vs nociceptive-pain reference), supporting the corrected label assignment.
Residual error magnitude is not reported in the paper. Equation 2 of the Methods describes the residual error as additive on log-transformed concentration with variance sigma^2, but the numerical sigma value is not given in Table 13 or anywhere in the main text or the 2018 correction. The model file uses
propSd = 0.20(~20 percent CV in linear space) as a documented placeholder - chosen as a mid-range popPK residual-error magnitude rather than a paper-derived value. Users running stochastic VPC simulations should either refitpropSdagainst their own data or interpret stochastic envelopes as illustrative only. The model is still suitable for deterministic typical-value predictions (usingrxode2::zeroRe()) because the residual error does not enter the typical-value forward solution.Reference-category implementation. The paper’s reference subject is “female, tablet formulation, unknown CYP2C9 phenotype, LBP/OA disease status, age 55 y, CrCl 106.4 mL/min, weight 82 kg, ALT 19 U/L.” The canonical
SEXFcovariate has reference 0 = male, but Kleideiter 2017 uses female as reference, so the model derives a male indicator insidemodel()as(1 - SEXF)and applies the male effectlog(87.4 / 74.3) = 0.162to it. Similarly, the canonicalCYP2C9_EM(reference 0 = IM/PM) does not natively express an “unknown” reference; the model pairs it with a newCYP2C9_PM_IMcompanion so that(CYP2C9_EM, CYP2C9_PM_IM) = (0, 0)represents the unknown-phenotype reference,(1, 0)represents EM, and(0, 1)represents the pooled PM/IM cohort. Both updates are documented ininst/references/covariate-columns.md.CrCl is raw Cockcroft-Gault, not BSA-normalized. Methods Section 2.4.1 states “Derived covariate creatinine CL (CrCl) was calculated from the observed data according to the Cockcroft-Gault formula.” This is the raw mL/min form, not the BSA-normalized mL/min/1.73 m^2 that the canonical
CRCLdefinition uses. The model file documents this incovariateData[[CRCL]]$notes; downstream users must supply raw Cockcroft-Gault values when using this model (matching the Delattre 2010 amikacin precedent).Concentration unit scaling. Cebranopadol dose is in ug and the apparent volumes are in L, so
central / vcnatively givesug/L = ng/mL. The paper reports concentrations in pg/mL, so the model multiplies by 1000 to match the published units. This is the only unit conversion in the model.Trial population details. Per-trial sex, age, and weight distributions are taken from Table 12; for cohorts whose individual covariates are not published, normally distributed perturbations around the trial-median values are used (10 percent CV for body weight, 10 percent CV for age, 15 percent CV for CrCl, 30 percent CV for ALT) to give the virtual cohort modest spread without inventing a covariate model.