Factor IX (Brekkan 2016)
Source:vignettes/articles/Brekkan_2016_factorIX.Rmd
Brekkan_2016_factorIX.RmdModel and source
- Citation: Brekkan A, Berntorp E, Jensen K, Nielsen EI, Jonsson S. Population pharmacokinetics of plasma-derived factor IX: procedures for dose individualization. J Thromb Haemost. 2016;14(4):724-732. doi:[10.1111/jth.13271](https://doi.org/10.1111/jth.13271)
- Description: Three-compartment population PK model for plasma-derived factor IX (FIX) activity in patients with moderate or severe haemophilia B.
- Article: https://doi.org/10.1111/jth.13271
- Modality: Plasma-derived FIX concentrate, IV infusion.
Brekkan 2016 reevaluated a previously published three-compartment popPK model for plasma-derived FIX activity (the “original model” of Berntorp et al., reference 15 in the paper) using an extended pooled data set, and used the refit to explore sparse sampling schedules for individual Bayesian dose prediction in haemophilia B. The packaged model implements the final re-estimated model (Brekkan 2016 Table 2, with equations in Material and methods, p. 725): three-compartment disposition with IV input and first-order elimination from the central compartment, allometric weight scaling on all CL / Q (exponent 0.75) and V (exponent 1.0) parameters with reference weight 70 kg, an endogenous FIX-activity baseline estimated as a structural parameter, two correlated IIV blocks (CL/V1 and V2/V3) plus an independent IIV on baseline, and a combined additive + proportional residual error. The final model has five fewer parameters than the original Berntorp model and an OFV 1941 points lower (Brekkan 2016 Results, p. 727).
Population
The development cohort comprised 34 unique patients with moderate or severe haemophilia B pooled across five previously published studies (Brekkan 2016 Table 1):
- 1,794 FIX activity samples; 7-17 samples per patient per occasion; 35 samples below the typical 0.01 U/mL limit of quantification were retained in the data set.
- Mean body weight 66.8 (SD 13.5) kg; per-study means 61.0-69.7 kg.
- Mean age 27.5 (SD 10.9) years; per-study means 23.1-42.8 years.
- Sex: haemophilia B is X-linked recessive, so the cohort is essentially all male.
- Race / ethnicity: not reported.
- Disease state: moderate or severe haemophilia B; baseline FIX activity estimated as a model parameter (0.01588 U/mL typical value).
- Products: seven plasma-derived FIX concentrates (AlphaNine - the most common - plus Factor IX Grifols, Immunine, Octanine, Nanotiv, Preconativ, Mononine). Product was tested as a covariate on CL and dropped from the final model because no product changed typical CL by more than 20% (Brekkan 2016 Results, p. 727).
- Sampling can in general be considered single-dose PK; the shortest and longest time periods between occasions were 4 days and > 4 years.
The Discussion notes the final model should be used with caution to
describe FIX activity following administration of products that are not
plasma-derived. The same metadata is available programmatically via
readModelDb("Brekkan_2016_factorIX")$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Brekkan_2016_factorIX.R. The
table below collects them in one place for review.
| Parameter (model name) | Value | Source |
|---|---|---|
lcl (typical CL, mL/h) |
log(319.8) | Brekkan 2016 Table 2: CL = 319.8 mL/h |
lvc (typical V1, mL) |
log(5922) | Brekkan 2016 Table 2: V1 = 5922 mL |
lvp (typical V2, mL) |
log(828.9) | Brekkan 2016 Table 2: V2 = 828.9 mL |
lq (typical Q2, mL/h) |
log(1049) | Brekkan 2016 Table 2: Q2 = 1049 mL/h |
lvp2 (typical V3, mL) |
log(2234) | Brekkan 2016 Table 2: V3 = 2234 mL |
lq2 (typical Q3, mL/h) |
log(160.4) | Brekkan 2016 Table 2: Q3 = 160.4 mL/h |
lrbase (endogenous baseline, U/mL) |
log(0.01588) | Brekkan 2016 Table 2: baseline FIX activity = 0.01588 U/mL |
| Allometric exponent on CL, Q2, Q3 | 0.75 (fixed) | Brekkan 2016 Methods p. 725 and Results p. 727 (three approaches gave similar fits) |
| Allometric exponent on V1, V2, V3 | 1.00 (fixed) | Brekkan 2016 Methods p. 725: volume exponent fixed at 1 |
| Reference body weight | 70 kg | Brekkan 2016 Table 2 footnote (typical value defined for 70 kg subject) |
IIV block etalcl + etalvc
|
c(0.016129, 0.014053, 0.024649) | Brekkan 2016 Table 2: x_CL = 0.127, x_V1 = 0.157, corr(CL,V1) = 0.705 |
IIV block etalvp + etalvp2
|
c(0.444889, 0.553828, 1.040400) | Brekkan 2016 Table 2: x_V2 = 0.667, x_V3 = 1.020, corr(V2,V3) = 0.814 |
etalrbase (IIV on baseline) |
0.042849 | Brekkan 2016 Table 2: x_BASELINE = 0.207 |
propSd (proportional residual) |
0.0695 | Brekkan 2016 Table 2: proportional residual error = 0.0695 |
addSd (additive residual, U/mL) |
0.0067 | Brekkan 2016 Table 2: additive residual error = 0.0067 U/mL |
Equation: d/dt(central)
|
n/a | Brekkan 2016 Material and methods, p. 725 (three-compartment IV model) |
Equation: d/dt(peripheral1)
|
n/a | Brekkan 2016 Material and methods, p. 725 |
Equation: d/dt(peripheral2)
|
n/a | Brekkan 2016 Material and methods, p. 725 |
Equation: Cc = central / vc + rbase
|
n/a | Brekkan 2016 Material and methods, p. 725 (baseline estimated as structural parameter) |
The IIV values are reported in Table 2 under the heading “coefficient
of variation of interindividual variability of clearance, volumes and
baseline”. The Brekkan 2016 paper does not include a
sqrt(variance) * 100 footnote directly, but the sister
factor IX papers from the same modelling lineage do (Diao 2014 Table 3
footnote: “IIV calculated as sqrt(variance) * 100”; Koopman 2023 Table 2
footnote: “IIV and IOV coefficient of variation calculated as:
sqrt(variance) * 100%”). Under that convention the reported value equals
the SD of the log-scale eta directly, so
omega^2 = (reported_value)^2 and
cov = corr * sqrt(var1) * sqrt(var2). This is the
convention encoded in the packaged model file. See Assumptions and
deviations for the small-IIV check.
The final model also estimated inter-occasion variability on CL (21.4% CV) and V1 (20.1% CV) with correlation 0.902 between the two random effects (Brekkan 2016 Table 2). IOV is not implemented in this static library model because the library event grid has no occasion variable; see Assumptions and deviations.
Virtual cohort
Original observed FIX activity data are not publicly available. The
simulations below use a virtual cohort whose demographics approximate
the Brekkan 2016 development population: body weight is sampled around
the cohort mean of 66.8 kg (capped to a plausible adult haemophilia B
range). Per Brekkan 2016 simulation design (p. 726) all simulated
patients are assigned a baseline FIX activity of 0 U/mL to represent
severe haemophilia B; this is implemented in the rxode2 call by
overriding rbase = 0.
set.seed(2016)
n_per_group <- 100L
cohort <- tibble(
ID = seq_len(n_per_group),
WT = pmin(pmax(rlnorm(n_per_group, log(66.8), 0.18), 45), 110),
treatment = "39 U/kg Mon+Thu"
)
stopifnot(!anyDuplicated(cohort$ID))
summary(cohort)
#> ID WT treatment
#> Min. : 1.00 Min. :45.00 Length :100
#> 1st Qu.: 25.75 1st Qu.:58.71 N.unique : 1
#> Median : 50.50 Median :63.67 N.blank : 0
#> Mean : 50.50 Mean :66.54 Min.nchar: 15
#> 3rd Qu.: 75.25 3rd Qu.:74.31 Max.nchar: 15
#> Max. :100.00 Max. :99.15The simulation replicates Brekkan 2016 Figure 1: eight 10-min IV infusions of 39 U/kg administered on Mondays and Thursdays (interval 72 h, then 96 h, alternating), with dense sampling after the eighth dose for 96 h. The 8th (final) dose is on the second Thursday of the third week (study day 24).
infusion_min <- 10
infusion_h <- infusion_min / 60
# Dose times in hours (relative to t = 0 on Monday of week 1):
# Mon week1 = 0; Thu week1 = 72; Mon week2 = 168; Thu week2 = 240;
# Mon week3 = 336; Thu week3 = 408; Mon week4 = 504; Thu week4 = 576.
dose_times <- c(0, 72, 168, 240, 336, 408, 504, 576)
last_dose <- max(dose_times)
# 22-point sampling schedule (Brekkan 2016 Fig. 1) after the last dose,
# expressed as hours after t = 0:
post_last <- c(0, 0.1, 0.5, 1, 2, 4, 6, 12, 18, 24, 30, 36,
42, 48, 54, 60, 66, 72, 78, 84, 90, 96)
obs_times <- last_dose + post_last
build_events <- function(pop) {
dose <- pop |>
tidyr::crossing(start = dose_times) |>
mutate(
AMT = WT * 39,
RATE = AMT / infusion_h,
TIME = start,
EVID = 1,
CMT = "central",
DV = NA_real_
) |>
select(-start)
obs <- pop |>
tidyr::crossing(TIME = obs_times) |>
mutate(AMT = NA_real_, RATE = NA_real_,
EVID = 0, CMT = "central", DV = NA_real_)
bind_rows(dose, obs) |>
arrange(ID, TIME, desc(EVID)) |>
as.data.frame()
}
events <- build_events(cohort)Simulation
Run a stochastic VPC-style simulation (between-subject variability on
CL, V1, V2, V3, and baseline) with rbase forced to 0 to
represent severe haemophilia B per the paper’s simulation design. A
typical-value simulation with the etas zeroed is included for parameter
back-checks.
mod <- readModelDb("Brekkan_2016_factorIX")
# Force baseline FIX activity to 0 (severe haemophilia B) per
# Brekkan 2016 p. 726: "In the simulations all patients were assumed to
# have a baseline FIX activity level of 0 (i.e. representing patients
# with severe hemophilia B)."
sim <- rxode2::rxSolve(
mod, events = events,
params = c(lrbase = -Inf),
keep = c("treatment", "WT"),
returnType = "data.frame"
)
#> ℹ parameter labels from comments will be replaced by 'label()'
sim <- sim[sim$time >= 0, ]
mod_typ <- rxode2::zeroRe(mod)
#> ℹ parameter labels from comments will be replaced by 'label()'
sim_typ <- rxode2::rxSolve(
mod_typ, events = events,
params = c(lrbase = -Inf),
keep = c("treatment", "WT"),
returnType = "data.frame"
)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalvp', 'etalvp2', 'etalrbase'
#> Warning: multi-subject simulation without without 'omega'
sim_typ <- sim_typ[sim_typ$time >= 0, ]Replicate Figure 1: FIX activity over the 24-day regimen
Brekkan 2016 Figure 1 shows the model-predicted FIX activity over the 24-day eight-infusion regimen for the simulation design. The figure below reproduces the typical-value profile, with the 5th-95th percentile envelope from the stochastic simulation overlaid.
sim_summary <- sim |>
filter(time >= 0) |>
group_by(time) |>
summarise(
median = stats::median(Cc, na.rm = TRUE),
lo = stats::quantile(Cc, 0.05, na.rm = TRUE),
hi = stats::quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_summary, aes(time / 24, median)) +
geom_ribbon(aes(ymin = lo, ymax = hi), alpha = 0.20, fill = "steelblue") +
geom_line(linewidth = 0.7, colour = "steelblue") +
geom_hline(yintercept = 0.01, linetype = "dashed", colour = "firebrick") +
annotate("text", x = 0.5, y = 0.012, label = "Target 0.01 U/mL",
colour = "firebrick", hjust = 0, size = 3) +
labs(
x = "Time after first dose (days)",
y = "FIX activity above baseline (U/mL)",
title = "Simulated plasma-derived FIX activity over the 24-day regimen",
subtitle = paste0("Median + 5-95% prediction interval (N = ", n_per_group,
"); 8 x 39 U/kg IV infusions Mon + Thu. ",
"Approximate analogue of Brekkan 2016 Figure 1."),
caption = "Model: Brekkan 2016 J Thromb Haemost 14(4):724-732"
) +
theme_bw()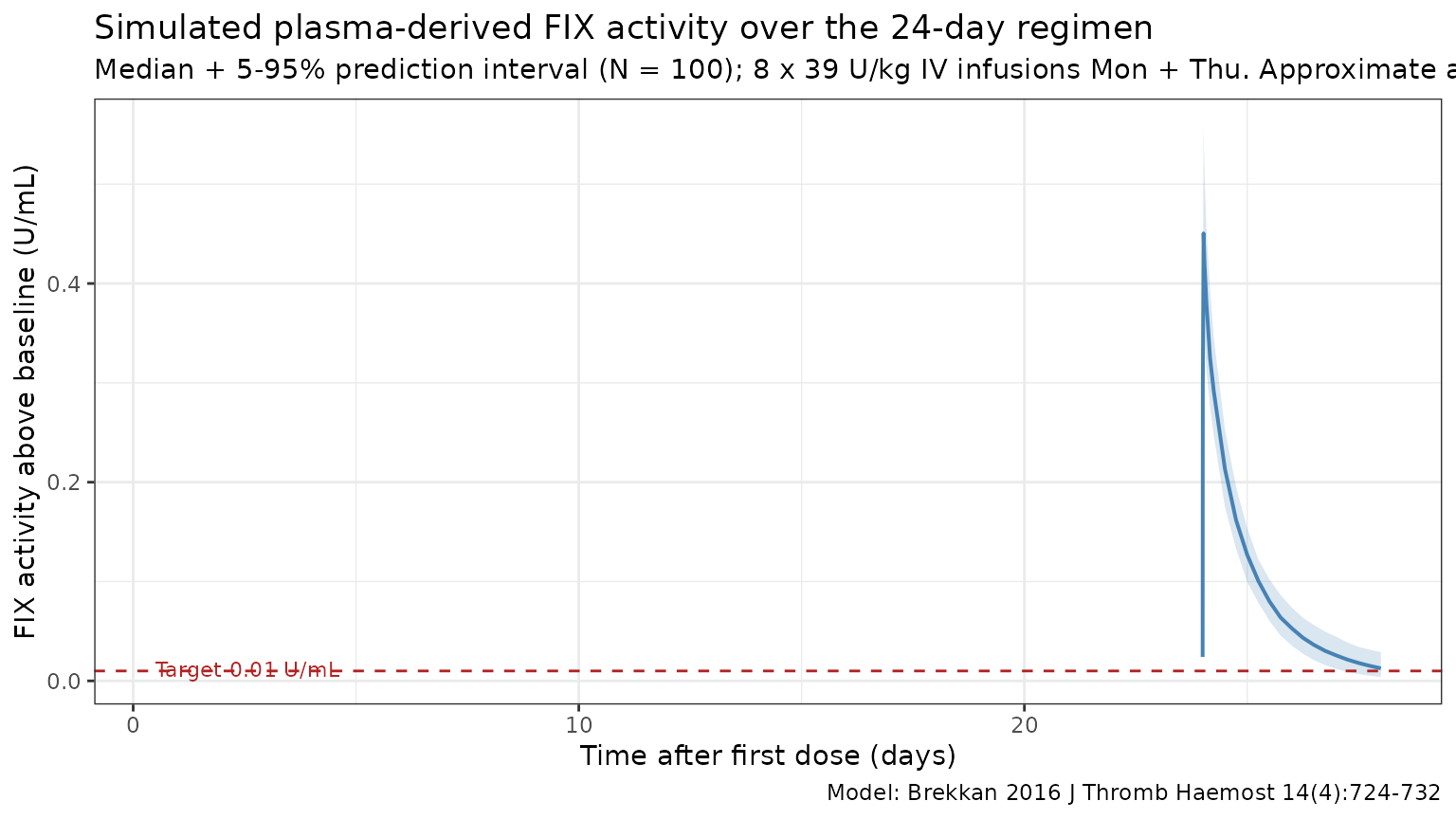
Trough back-check at 96 h after the eighth dose
Brekkan 2016 p. 726 fixes the simulation dose (39 U/kg) by the
criterion that “it resulted in a trough FIX activity level of 0.01 U
mL-1 in a patient with a body weight of 70 kg.” The check below
evaluates that trough in the typical-value simulation
(zeroRe() + rbase = 0) for a 70 kg
subject.
mod_typ_70 <- rxode2::zeroRe(mod)
#> ℹ parameter labels from comments will be replaced by 'label()'
events_70 <- build_events(tibble(ID = 1L, WT = 70, treatment = "70 kg ref"))
sim_typ_70 <- rxode2::rxSolve(
mod_typ_70, events = events_70,
params = c(lrbase = -Inf),
returnType = "data.frame"
)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalvp', 'etalvp2', 'etalrbase'
trough_row <- sim_typ_70[sim_typ_70$time == last_dose + 96, ]
trough_val <- trough_row$Cc
knitr::kable(
data.frame(
quantity = c("Trough at 96 h after dose 8 (typical, 70 kg, 39 U/kg)",
"Brekkan 2016 target trough"),
value_U_per_mL = c(round(trough_val, 4), 0.01)
),
caption = "Typical-value trough check for the dose-individualisation design.",
align = c("l", "r")
)| quantity | value_U_per_mL |
|---|---|
| Trough at 96 h after dose 8 (typical, 70 kg, 39 U/kg) | 0.0127 |
| Brekkan 2016 target trough | 0.0100 |
Typical CL and Vss back-check
Brekkan 2016 Table 2 reports the structural parameters for a typical 70 kg subject. Reproducing those numbers from a single-bolus typical-value simulation is the simplest self-consistency check (Vss = V1 + V2 + V3).
ev_ref <- rxode2::et(amt = 50 * 70, time = 0, cmt = "central") |>
rxode2::et(0)
sim_ref <- rxode2::rxSolve(
mod_typ, events = ev_ref,
params = c(WT = 70, lrbase = -Inf),
returnType = "data.frame"
)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalvp', 'etalvp2', 'etalrbase'
ref_pars <- sim_ref[1, c("cl", "vc", "q", "vp", "q2", "vp2"), drop = FALSE]
ref_pars$Vss <- ref_pars$vc + ref_pars$vp + ref_pars$vp2
knitr::kable(
ref_pars,
caption = "Typical-value PK parameters for the reference 70 kg patient (mL, mL/h).",
digits = c(2, 1, 2, 2, 2, 2, 1)
)| cl | vc | q | vp | q2 | vp2 | Vss |
|---|---|---|---|---|---|---|
| 319.8 | 5922 | 1049 | 828.9 | 160.4 | 2234 | 8984.9 |
The model returns CL = 319.8 mL/h, V1 = 5922 mL, Q2 = 1049 mL/h, V2 = 828.9 mL, Q3 = 160.4 mL/h, V3 = 2234 mL, and Vss = V1 + V2 + V3 = 8985 mL — matching the values reported in Brekkan 2016 Table 2 (CL = 319.8 mL/h, V1 = 5922 mL, Q2 = 1049 mL/h, V2 = 828.9 mL, Q3 = 160.4 mL/h, V3 = 2234 mL, Vss = 8985 mL).
PKNCA validation: single-dose summary
Brekkan 2016 does not tabulate single-dose NCA parameters directly; the paper’s quantitative results are framed in terms of dose-individualisation performance rather than NCA descriptors. The PKNCA summary below provides the standard NCA descriptors (Cmax, AUC0-inf, terminal half-life) on a single-dose schedule for context.
single_events <- cohort |>
mutate(AMT = WT * 50) |>
tidyr::crossing(TIME = c(0, c(0.1, 0.5, 1, 2, 4, 6, 12, 18, 24,
30, 36, 42, 48, 54, 60, 66, 72,
78, 84, 90, 96, 120, 144, 168, 240, 336))) |>
mutate(
EVID = if_else(TIME == 0, 1L, 0L),
AMT = if_else(TIME == 0, AMT, NA_real_),
RATE = if_else(TIME == 0, AMT / infusion_h, NA_real_),
CMT = "central",
DV = NA_real_
) |>
arrange(ID, TIME, desc(EVID)) |>
as.data.frame()
sim_single <- rxode2::rxSolve(
mod, events = single_events,
params = c(lrbase = -Inf),
keep = c("treatment", "WT"),
returnType = "data.frame"
)
sim_single <- sim_single[sim_single$time >= 0, ]
sim_nca <- sim_single |>
filter(!is.na(Cc)) |>
select(id, time, Cc, treatment)
# Guarantee a time=0 row per (id, treatment); IV bolus pre-dose Cc=0.
sim_nca <- bind_rows(
sim_nca,
sim_nca |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
dose_df <- single_events |>
filter(EVID == 1) |>
transmute(id = ID, time = TIME, amt = AMT, treatment)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id,
concu = "U/mL",
timeu = "h")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id,
doseu = "U")
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE,
clast.obs = TRUE,
lambda.z = TRUE
)
nca_res <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_obj, dose_obj,
intervals = intervals))
nca_tbl <- as.data.frame(nca_res$result)
summary_by_param <- function(param) {
nca_tbl |>
filter(PPTESTCD == param) |>
group_by(treatment) |>
summarise(
n = sum(!is.na(PPORRES)),
median = stats::median(PPORRES, na.rm = TRUE),
q05 = stats::quantile(PPORRES, 0.05, na.rm = TRUE),
q95 = stats::quantile(PPORRES, 0.95, na.rm = TRUE),
.groups = "drop"
)
}
nca_summary <- bind_rows(
summary_by_param("cmax") |> mutate(parameter = "Cmax (U/mL)"),
summary_by_param("tmax") |> mutate(parameter = "Tmax (h)"),
summary_by_param("aucinf.obs") |> mutate(parameter = "AUC0-inf (U*h/mL)"),
summary_by_param("half.life") |> mutate(parameter = "Terminal half-life (h)")
) |>
select(parameter, n, median, q05, q95)
knitr::kable(
nca_summary,
caption = "Simulated plasma-derived FIX NCA after a single 50 U/kg IV infusion.",
digits = c(0, 0, 3, 3, 3)
)| parameter | n | median | q05 | q95 |
|---|---|---|---|---|
| Cmax (U/mL) | 100 | 0.519 | 0.416 | 0.696 |
| Tmax (h) | 100 | 0.500 | 0.500 | 0.500 |
| AUC0-inf (U*h/mL) | 100 | 10.585 | 8.500 | 12.911 |
| Terminal half-life (h) | 100 | 22.503 | 13.328 | 56.924 |
Errata
No published erratum was located for Brekkan 2016 (J Thromb Haemost 2016;14(4):724-732). The packaged parameter values are taken from Brekkan 2016 Table 2 (final model), which is internally consistent with the equations on p. 725 and the simulation design on p. 726.
Assumptions and deviations
-
Inter-occasion variability omitted. Brekkan 2016
estimated IOV on CL (21.4% CV) and V1 (20.1% CV) with a correlation of
0.902 between the two random effects (Table 2). The static library model
has no occasion variable, so IOV is not implemented as a separate eta.
For Bayesian forecasting use cases that explicitly model occasions, the
IOV variances (
omega^2_IOV_CL = 0.214^2 = 0.045796andomega^2_IOV_V1 = 0.201^2 = 0.040401, covariance0.902 * 0.214 * 0.201 = 0.038804) can be added on top of the packaged IIV. -
Inter-individual variability convention. Brekkan
2016 does not state the IIV definition formula directly in the Table 2
footnote, but the related factor IX papers from the same modelling
lineage (Diao 2014 Table 3 footnote; Koopman 2023 Table 2 footnote) both
define the IIV column as
sqrt(variance) * 100, i.e. the reported value equals the SD of the log-scale eta directly. The packaged variances were computed withomega^2 = (reported_value)^2and covariances ascorr * sqrt(var1) * sqrt(var2)to match this convention. For the small IIVs (x_CL = 0.127,x_V1 = 0.157) the two interpretations (omega^2 = reported^2vs.omega^2 = log(reported^2 + 1)) differ by less than 1%; for the large IIV on V3 (x_V3 = 1.020) they differ by ~30%, which is the dominant uncertainty in any user-facing simulation of the terminal-phase variability. -
No IIV on Q2 or Q3. Brekkan 2016 retained five
fewer parameters than the original Berntorp model after model
simplification, dropping IIV on Q2 and Q3 (Results, p. 727: “the
original model could be reduced by four parameters related to the IIV
part”). The packaged model carries no
etalqoretalq2. -
Endogenous baseline FIX activity. Brekkan 2016 fits
the baseline FIX activity as a structural parameter rather than
baseline-correcting the observations. The model output
Cc = central / vc + rbasetherefore represents total measured FIX activity (exogenous-attributable + endogenous baseline). To represent severe haemophilia B (the simulation design of Brekkan 2016 p. 726), setrbase = 0by passingparams = c(lrbase = -Inf)torxSolve()(as used in the simulations in this vignette). To represent a patient with moderate haemophilia B and endogenous activity, leavelrbaseat its default value. -
Allometric exponents fixed at theoretical values.
Brekkan 2016 Methods p. 725 fixes the body weight exponent at 1 for
volumes and 0.75 for intercompartmental CL parameters; Results p. 727
fixes the exponent on CL at 0.75 after evaluating three approaches
(estimated, fixed at 1.26 from the original Berntorp model, fixed at
0.75) that all gave similar fits. The packaged
model()block multiplies CL, Q2, Q3 by(WT / 70)^0.75and V1, V2, V3 by(WT / 70)^1.00. - FIX product covariate omitted. Brekkan 2016 tested seven plasma- derived FIX products as a categorical covariate on CL. The likelihood- ratio test was statistically significant (P < 0.01, df = 6) but the largest deviation from AlphaNine was within +/- 20% of the typical CL (range 252-378 mL/h vs. 315 mL/h reference), so the clinical-significance criterion was not met and the product effect was dropped from the final model (Brekkan 2016 Results, p. 727). The Discussion notes the final model “should be used with caution to describe the FIX activity following administration of products that are not plasma-derived.”
- Age covariate omitted. Brekkan 2016 tested age as a fractional-change effect on CL (Equation 2 in the paper) and found it not statistically significant. The Discussion notes that incorporating body weight in the model explains part of the variability related to age.
- Virtual cohort. Body weight was sampled from a log-normal distribution centred at the cohort mean (66.8 kg) and capped at a plausible adult haemophilia B range (45-110 kg). The empirical body weight distribution in Brekkan 2016 (per-study means 61.0-69.7 kg, overall SD 13.5 kg) is approximated, not exactly reproduced.
-
Haemophilia B is X-linked recessive, so the
development cohort and the virtual cohort here are essentially all male
(
sex_female_pct = 0in the population metadata). The model has no sex covariate.