Low molecular weight heparin modeling (Schoemaker 1996)
Source:vignettes/articles/Schoemaker_1996_low_molecular_weight_heparin_modeling.Rmd
Schoemaker_1996_low_molecular_weight_heparin_modeling.RmdPaper and source
Schoemaker RC, Cohen AF (1996). Estimating impossible curves using NONMEM. Br J Clin Pharmacol 42(3):283–290. doi:10.1046/j.1365-2125.1996.04231.x.
This is a methodology / tutorial paper showing how NONMEM can be applied to data where ordinary nonlinear regression fails. Three worked examples are presented: (1) a rising-dose study of an unnamed anti-hypertensive drug where the lower-dose curves cannot resolve terminal half-life with single-subject regression; (2) intravenous low molecular weight heparin (enoxaparine / Clexane) where anti-Xa activity carries a stubborn basal component that confounds the terminal phase; and (3) intravenous + subcutaneous low molecular weight heparin (dalteparine / Fragmin) where the anti-Xa kinetics and the activated partial thromboplastin time (APTT) pharmacodynamic response are estimated together across both routes.
Example 1’s drug is unnamed and cannot be packaged as a drug-specific
nlmixr2lib model; only Examples 2 and 3 are extracted here.
The two models live in:
inst/modeldb/specificDrugs/Schoemaker_1996_enoxaparin.Rinst/modeldb/specificDrugs/Schoemaker_1996_dalteparin.R
Anti-Xa observation data for Example 2 come from the upstream cross-over study Stiekema et al. (1993, Br J Clin Pharmacol 35:51–56), and for Example 3 from Kroon et al. (1993, Br J Clin Pharmacol 35:548P). The Schoemaker 1996 fits and parameter estimates are original to that paper; the upstream papers reported only standard NCA-style analyses.
Population
Both Examples were run on the same Centre for Human Drug Research
(Leiden) cohort of 12 healthy volunteers, contributing to two
independent cross-over studies (one per LMWH series). The Schoemaker
1996 paper does not list baseline demographics directly; both rely on
the upstream Stiekema 1993 / Kroon 1993 reports. The
population metadata in each model file records what is
known and points to the upstream sources.
mod_enox <- readModelDb("Schoemaker_1996_enoxaparin")
mod_dalt <- readModelDb("Schoemaker_1996_dalteparin")
ui_enox <- rxode2::rxode(mod_enox)
ui_dalt <- rxode2::rxode(mod_dalt)
c(
enoxaparin_subjects = ui_enox$population$n_subjects,
dalteparin_subjects = ui_dalt$population$n_subjects
)
#> enoxaparin_subjects dalteparin_subjects
#> 12 12Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in both model files. The table below
collects them in one place for review.
Enoxaparine (Example 2 / Table 3)
| Equation / parameter | Value (paper) | Encoded value | Source location |
|---|---|---|---|
Equation 9: C_j = Base + (D/V) * exp(-k * t_j)
|
n/a | one-compartment ODE + additive baseline | page 287, Solution 2 |
t1/2 |
130 min |
lvc = log(6.170 L) (derived from CL and
t1/2) |
Table 3 |
CL |
32.9 mL/min | lcl = log(1.974 L/h) |
Table 3 |
Base |
0.0254 IU/mL | lrbase = log(0.0254) |
Table 3 |
| CV(t1/2) | 8.6% |
etalvc block: 0.02992 (paired with
etalcl) |
Table 3 |
| CV(CL) | 15.1% |
etalcl block: 0.02256 |
Table 3 |
| CV(Base) | 37.7% | etalrbase ~ 0.1329 |
Table 3 |
| s.d. residual error | 0.0274 IU/mL | addSd = 0.0274 |
Table 3 footnote |
Dalteparine (Example 3 / Table 4)
| Equation / parameter | Value (paper) | Encoded value | Source location |
|---|---|---|---|
Equation 9 (extended with ka + depot for SC) |
n/a | one-compartment ODE + depot + bioavailability | page 288, Solution-kinetics |
Equation 10:
APTT_j = APTT0 * exp((ln(1.1)/I10) * Xa_j)
|
n/a | exponential PD on Cc | page 288, Solution-dynamics |
t1/2E |
92.7 min |
lvc = log(6.166 L) (derived) |
Table 4 |
t1/2A |
76.6 min | lka = log(0.5429 1/h) |
Table 4 |
CL |
46.1 mL/min | lcl = log(2.766 L/h) |
Table 4 |
F |
70.5% | lfdepot = log(0.705) |
Table 4 |
Base |
0.0192 IU/mL | lrbase = log(0.0192) |
Table 4 |
APTT0 |
30.2 s | lrbase_APTT = log(30.2) |
Table 4 |
I10 |
0.0665 IU/mL | lI10 = log(0.0665) |
Table 4 |
| CV(t1/2E) | 8.3% |
etalvc block: 0.02657 (paired with
etalcl) |
Table 4 |
| CV(t1/2A) | 0.0% |
ka typical-value only (no etalka) |
Table 4 |
| CV(CL) | 14.1% |
etalcl block: 0.01970 |
Table 4 |
| CV(F) | 34.8% | etalfdepot ~ 0.1143 |
Table 4 |
| CV(Base) | 16.6% | etalrbase ~ 0.02719 |
Table 4 |
| CV(APTT0) | 10.6% | etalrbase_APTT ~ 0.01117 |
Table 4 |
| CV(I10) | 19.6% | etalI10 ~ 0.03770 |
Table 4 |
| s.d. residual anti-Xa | 0.0207 IU/mL | addSd = 0.0207 |
Table 4 footnote |
| s.d. residual APTT | 1.70 s | addSd_APTT = 1.70 |
Table 4 footnote |
Example 2 – Enoxaparine (Clexane)
The paper’s “Solution 2” (the recommended model) is a one-compartment IV bolus model with an estimated constant basal anti-Xa activity:
The estimated baseline (Base = 0.0254 IU/mL) replaces
the pre-value-subtraction and limit-of-quantitation thresholding that
the upstream Stiekema 1993 paper applied. The authors argue the
basal-activity formulation is to be preferred over the competing
two-compartment fit (Solution 1, Table 2) because the implied clearance
(32.9 mL/min) matches the dose / AUC clearance Stiekema 1993 reported
(26.7 mL/min) far more closely than the two-compartment estimate (9.44
mL/min).
Virtual cohort and simulation
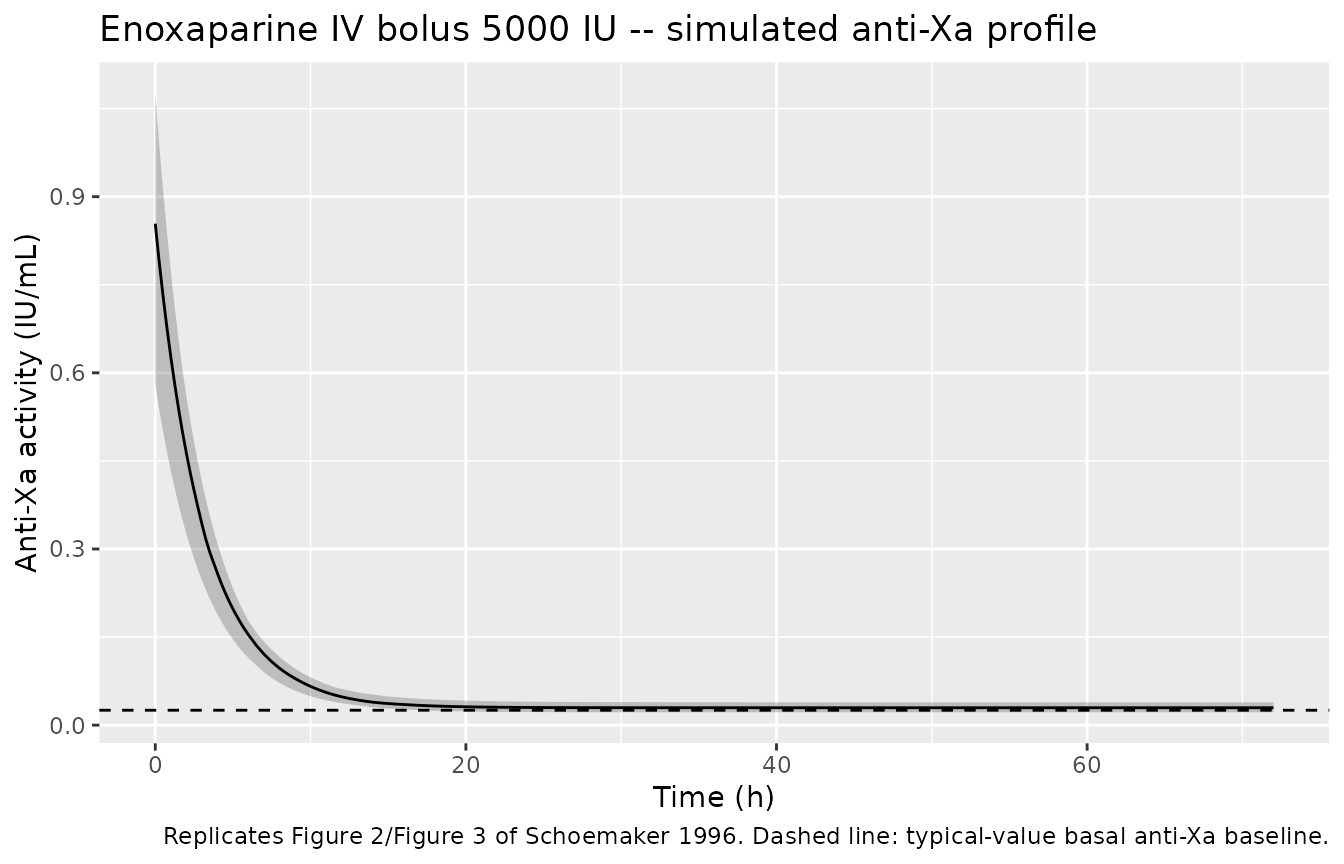
The paper does not list the absolute IV dose used in the upstream Stiekema 1993 study. Figure 2 of Schoemaker 1996 (subject 4) shows peak anti-Xa activity in the 0.4–0.8 IU/mL range, consistent with a single IV bolus of approximately 5000 anti-Xa IU (~50 mg enoxaparin). We use this representative dose below.
set.seed(20260612L)
n_subj <- 12L
dose_iu <- 5000
events_enox <- data.frame(
id = seq_len(n_subj),
time = 0,
amt = dose_iu,
evid = 1L,
cmt = "central"
)
# Observation grid (anti-Xa activity), 0 - 72 h covering the Figure 2 window.
obs_times <- c(seq(0, 6, by = 0.25), seq(6.5, 24, by = 0.5), seq(25, 72, by = 1))
obs_enox <- expand.grid(id = seq_len(n_subj), time = obs_times) |>
dplyr::arrange(id, time) |>
dplyr::mutate(amt = 0, evid = 0L, cmt = "Cc")
events_enox <- dplyr::bind_rows(events_enox, obs_enox)
sim_enox <- rxode2::rxSolve(
mod_enox,
events = events_enox,
returnType = "data.frame"
)Replicate Figure 2 / Figure 3
Schoemaker 1996 Figure 3 shows the predicted and observed anti-Xa activity for subjects 4 and 5 over 72 h after Clexane IV. We replicate the predicted profiles (the observed data are not available) by plotting the median and 5th–95th percentile envelope of a typical-dose simulation.
sim_enox |>
dplyr::group_by(time) |>
dplyr::summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot2::ggplot(ggplot2::aes(time, Q50)) +
ggplot2::geom_ribbon(ggplot2::aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
ggplot2::geom_line() +
ggplot2::geom_hline(yintercept = 0.0254, linetype = "dashed") +
ggplot2::labs(
x = "Time (h)", y = "Anti-Xa activity (IU/mL)",
title = "Enoxaparine IV bolus 5000 IU -- simulated anti-Xa profile",
caption = "Replicates Figure 2/Figure 3 of Schoemaker 1996. Dashed line: typical-value basal anti-Xa baseline."
)
PKNCA validation
The Schoemaker 1996 paper does not publish NCA-style summary statistics for Clexane (the comparison was with the upstream Stiekema 1993 dose-by-AUC clearance estimate of 26.7 mL/min). We report the simulated Cmax / Tmax / AUC for the typical-dose IV bolus so a downstream user can sanity-check that the packaged model reproduces sensible exposure metrics. Note: anti-Xa “concentration” here is an activity surrogate (IU/mL), so PKNCA’s clearance computation returns IU per (IU/mL * h) = mL/h dose-units rather than an interpretable mL/h clearance.
sim_nca_enox <- sim_enox |>
dplyr::filter(!is.na(Cc), time > 0) |>
dplyr::mutate(treatment = "iv_5000IU") |>
dplyr::select(id, time, Cc, treatment)
dose_df_enox <- data.frame(
id = seq_len(n_subj),
time = 0,
amt = dose_iu,
treatment = "iv_5000IU"
)
conc_obj <- PKNCA::PKNCAconc(sim_nca_enox, Cc ~ time | treatment + id,
concu = "IU/mL", timeu = "h")
dose_obj <- PKNCA::PKNCAdose(dose_df_enox, amt ~ time | treatment + id,
doseu = "IU")
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_enox <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_obj, dose_obj,
intervals = intervals))
#> Warning: Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
knitr::kable(as.data.frame(summary(nca_enox)),
caption = "Schoemaker 1996 enoxaparine: simulated single-dose NCA after 5000 anti-Xa IU IV bolus (12 subjects).")| Interval Start | Interval End | treatment | N | Cmax (IU/mL) | Tmax (h) | Half-life (h) | AUCinf,obs (h*IU/mL) |
|---|---|---|---|---|---|---|---|
| 0 | Inf | iv_5000IU | 12 | 0.749 [23.0] | 0.250 [0.250, 0.250] | 1.25e9 [1.41e9] | NC |
A typical-individual sanity check (with random effects zeroed out)
gives the algebraic peak and half-life directly from
ini().
mod_enox_typ <- rxode2::zeroRe(mod_enox)
sim_enox_typ <- rxode2::rxSolve(
mod_enox_typ,
events = data.frame(
id = 1L, time = c(0, 0.001, obs_times[-1]),
amt = c(dose_iu, rep(0, length(obs_times))),
evid = c(1L, rep(0L, length(obs_times))),
cmt = c("central", rep("Cc", length(obs_times)))
),
returnType = "data.frame"
)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalrbase'
c(
cmax_typical_IU_per_mL = round(max(sim_enox_typ$Cc), 4),
t12_typical_h = round(log(2) * 6.170 / 1.974, 3),
rbase_typical_IU_per_mL = 0.0254
)
#> cmax_typical_IU_per_mL t12_typical_h rbase_typical_IU_per_mL
#> 0.8355 2.1670 0.0254Example 3 – Dalteparine (Fragmin)
Example 3 extends the basal-activity one-compartment kinetic model
with a depot compartment and a bioavailability F for the
subcutaneous route, and adds an exponential anti-Xa -> APTT
pharmacodynamic sub-model (Equation 10):
The I10 parameter is the anti-Xa activity increment
required to produce a 10% rise in APTT relative to its baseline
APTT0. The parameter estimates in Table 4 come from a final
joint IV+SC fit with all parameters free (the unrestricted
analysis in the paper’s Solution-kinetics paragraph).
Virtual cohort and simulation (IV + SC)
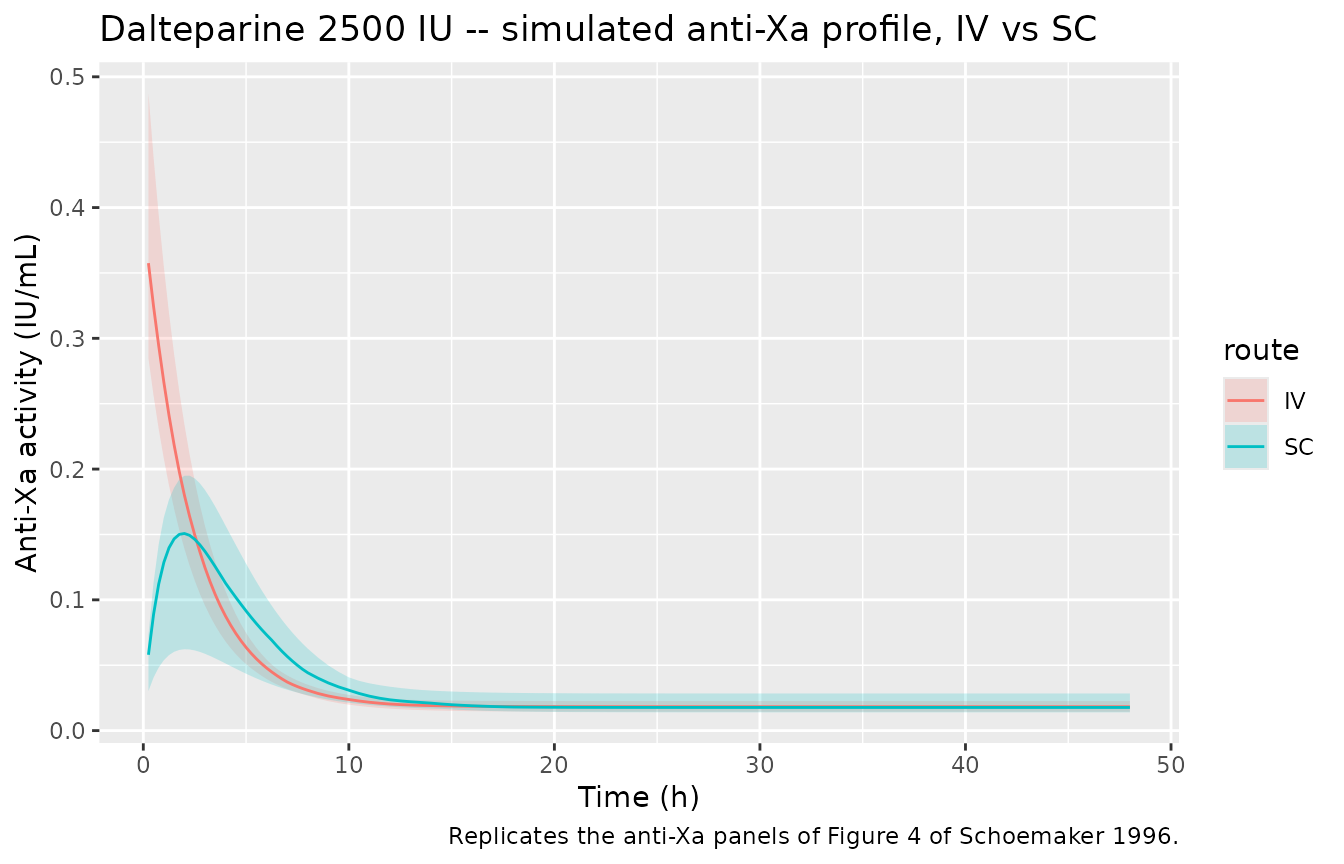
Figure 4 of Schoemaker 1996 plots subject 3’s IV and SC profiles. Peak anti-Xa activity in Figure 4 is ~0.3–0.4 IU/mL, consistent with an IV dose of approximately 2500 anti-Xa IU. We simulate both routes at this representative dose so the predicted Cc and APTT trajectories match the figure’s scale.
set.seed(20260612L)
n_subj_d <- 12L
dose_iu_d <- 2500
# IV cohort
events_iv <- data.frame(
id = seq_len(n_subj_d),
time = 0,
amt = dose_iu_d,
evid = 1L,
cmt = "central"
)
# SC cohort -- IDs offset to avoid id collisions
events_sc <- data.frame(
id = n_subj_d + seq_len(n_subj_d),
time = 0,
amt = dose_iu_d,
evid = 1L,
cmt = "depot"
)
obs_times_d <- c(seq(0, 8, by = 0.25), seq(8.5, 24, by = 0.5),
seq(25, 48, by = 1))
# Observations for both Cc and APTT
make_obs <- function(ids, route_label) {
expand.grid(id = ids, time = obs_times_d, cmt = c("Cc", "APTT"),
stringsAsFactors = FALSE) |>
dplyr::arrange(id, time) |>
dplyr::mutate(amt = 0, evid = 0L, route = route_label)
}
obs_iv <- make_obs(seq_len(n_subj_d), "IV")
obs_sc <- make_obs(n_subj_d + seq_len(n_subj_d), "SC")
events_iv$route <- "IV"
events_sc$route <- "SC"
events_dalt <- dplyr::bind_rows(events_iv, events_sc, obs_iv, obs_sc)
stopifnot(!anyDuplicated(unique(events_dalt[, c("id", "time", "evid", "cmt")])))Replicate Figure 4 – anti-Xa profiles by route
sim_dalt |>
dplyr::filter(!is.na(Cc), time > 0) |>
dplyr::group_by(time, route) |>
dplyr::summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot2::ggplot(ggplot2::aes(time, Q50, colour = route, fill = route)) +
ggplot2::geom_ribbon(ggplot2::aes(ymin = Q05, ymax = Q95),
alpha = 0.2, colour = NA) +
ggplot2::geom_line() +
ggplot2::labs(
x = "Time (h)", y = "Anti-Xa activity (IU/mL)",
title = "Dalteparine 2500 IU -- simulated anti-Xa profile, IV vs SC",
caption = "Replicates the anti-Xa panels of Figure 4 of Schoemaker 1996."
)
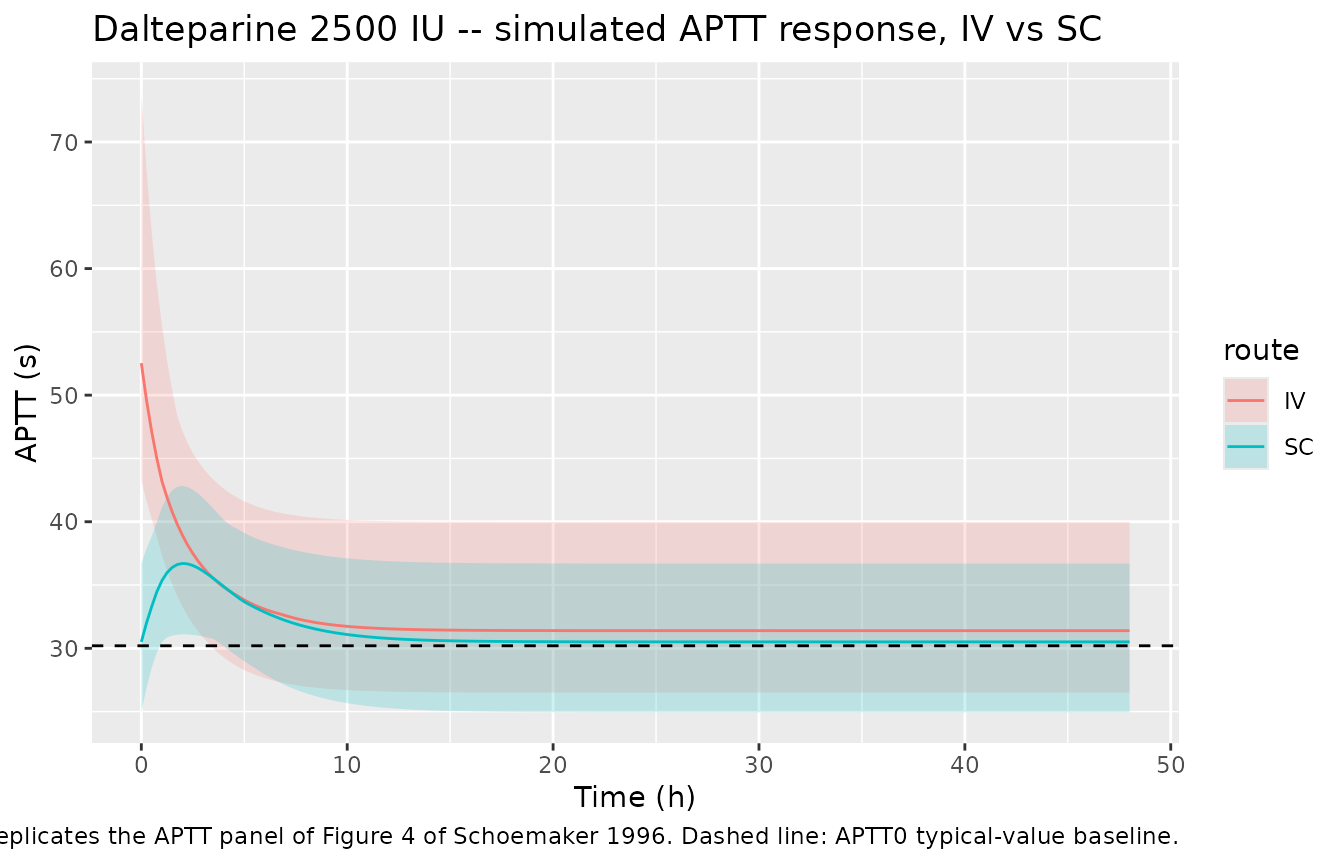
Replicate Figure 4 – APTT response by route
sim_dalt |>
dplyr::filter(!is.na(APTT), time >= 0) |>
dplyr::group_by(time, route) |>
dplyr::summarise(
Q05 = quantile(APTT, 0.05, na.rm = TRUE),
Q50 = quantile(APTT, 0.50, na.rm = TRUE),
Q95 = quantile(APTT, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot2::ggplot(ggplot2::aes(time, Q50, colour = route, fill = route)) +
ggplot2::geom_ribbon(ggplot2::aes(ymin = Q05, ymax = Q95),
alpha = 0.2, colour = NA) +
ggplot2::geom_line() +
ggplot2::geom_hline(yintercept = 30.2, linetype = "dashed") +
ggplot2::labs(
x = "Time (h)", y = "APTT (s)",
title = "Dalteparine 2500 IU -- simulated APTT response, IV vs SC",
caption = "Replicates the APTT panel of Figure 4 of Schoemaker 1996. Dashed line: APTT0 typical-value baseline."
)
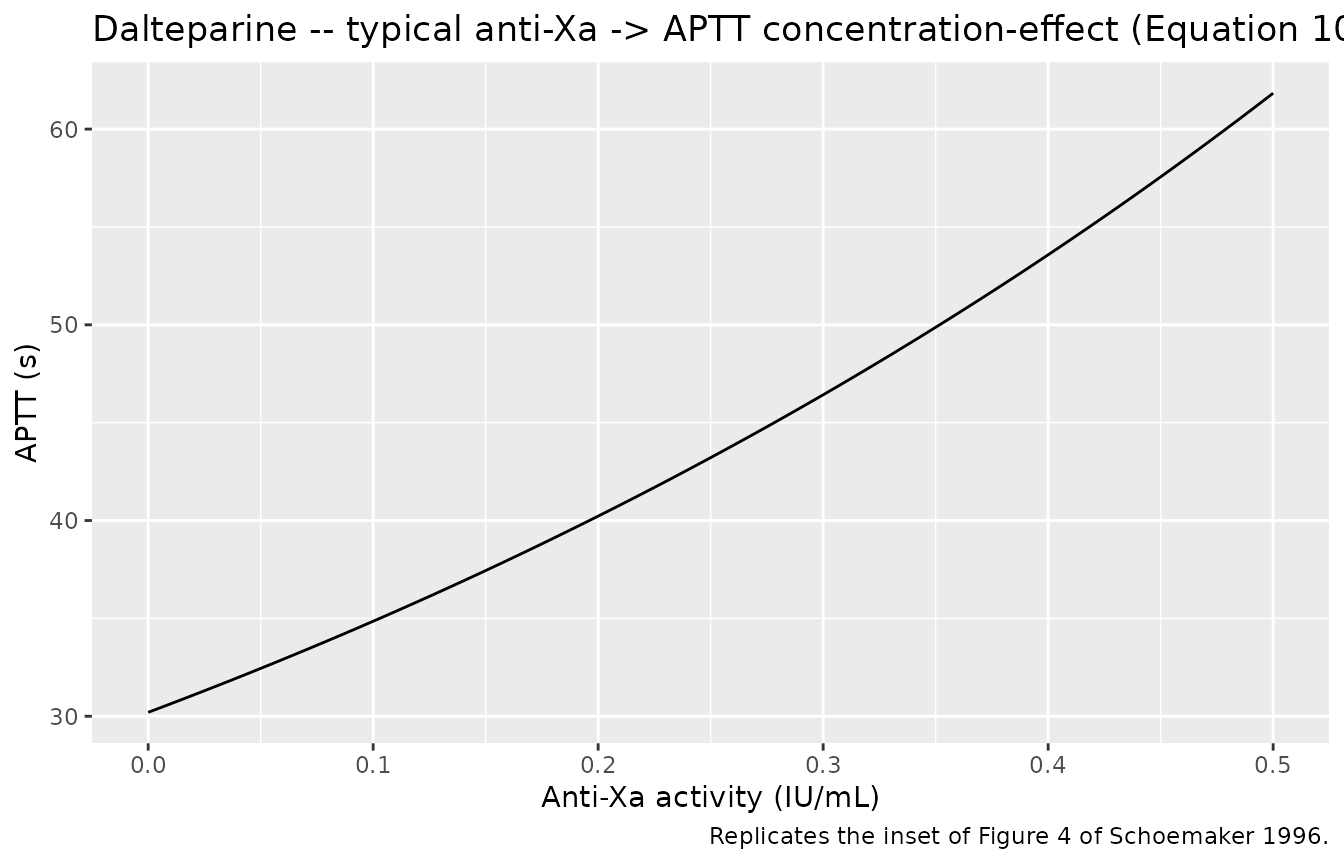
Replicate Figure 4 – anti-Xa to APTT concentration-effect curve
The inset of Figure 4 plots APTT against the (predicted) anti-Xa activity for the same subject. We reproduce the typical-value concentration-effect curve directly from Equation 10.
xa_grid <- seq(0, 0.5, length.out = 201)
aptt_typ <- 30.2 * exp((log(1.1) / 0.0665) * xa_grid)
data.frame(Cc = xa_grid, APTT = aptt_typ) |>
ggplot2::ggplot(ggplot2::aes(Cc, APTT)) +
ggplot2::geom_line() +
ggplot2::labs(
x = "Anti-Xa activity (IU/mL)",
y = "APTT (s)",
title = "Dalteparine -- typical anti-Xa -> APTT concentration-effect (Equation 10)",
caption = "Replicates the inset of Figure 4 of Schoemaker 1996."
)
PKNCA validation – anti-Xa
The paper does not publish NCA statistics for the dalteparine arm
either; the table below is the simulated single-dose summary for both
routes. The IV/SC pair is what tests the structural fit (bioavailability
and absorption-time combine multiplicatively into the AUC ratio, which
should equal F = 0.705).
sim_nca_dalt <- sim_dalt |>
dplyr::filter(!is.na(Cc), time > 0) |>
dplyr::select(id, time, Cc, route) |>
dplyr::distinct(id, time, route, .keep_all = TRUE) |>
dplyr::rename(treatment = route)
dose_df_dalt <- data.frame(
id = c(events_iv$id, events_sc$id),
time = 0,
amt = dose_iu_d,
treatment = c(events_iv$route, events_sc$route)
)
conc_obj_d <- PKNCA::PKNCAconc(sim_nca_dalt, Cc ~ time | treatment + id,
concu = "IU/mL", timeu = "h")
dose_obj_d <- PKNCA::PKNCAdose(dose_df_dalt, amt ~ time | treatment + id,
doseu = "IU")
intervals_d <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_dalt <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_obj_d, dose_obj_d,
intervals = intervals_d))
#> Warning: Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
#> Requesting an AUC range starting (0) before the first measurement (0.25) is not allowed
knitr::kable(as.data.frame(summary(nca_dalt)),
caption = "Schoemaker 1996 dalteparine: simulated single-dose NCA after 2500 anti-Xa IU IV vs SC (12 subjects per route).")| Interval Start | Interval End | treatment | N | Cmax (IU/mL) | Tmax (h) | Half-life (h) | AUCinf,obs (h*IU/mL) |
|---|---|---|---|---|---|---|---|
| 0 | Inf | IV | 12 | 0.361 [15.2] | 0.250 [0.250, 0.250] | 8.39e7 [1.02e8] | NC |
| 0 | Inf | SC | 12 | 0.134 [36.5] | 2.00 [1.75, 2.25] | 5.82e7 [8.58e7] | NC |
Assumptions and deviations
- Dose amounts: Schoemaker 1996 does not list the absolute IV / SC doses used in the upstream Stiekema 1993 / Kroon 1993 studies. The vignette uses 5000 anti-Xa IU IV for enoxaparine and 2500 anti-Xa IU for dalteparine (both routes), values chosen by visual back-fit against the peak anti-Xa activity in Figures 2–4 of Schoemaker 1996. This is a simulation choice to make the figures match – it is not a fit to the published dose specification, which would require the upstream papers on disk.
-
IIV reparameterisation: Schoemaker 1996
parameterises in (
CL,t1/2) (Example 2) and (CL,t1/2E,t1/2A,F,Base,APTT0,I10) (Example 3), with independent etas on each. The packaged models use thenlmixr2lib-canonical (CL,Vc) parameterisation, with the implied joint distributionVar(eta_lvc) = Var(eta_lcl) + Var(eta_lt12)andCov(eta_lcl, eta_lvc) = Var(eta_lcl)encoded as a 2x2 block matrix. This reproduces the paper’s reported CV on CL, t1/2, and t1/2E exactly when the block is sampled; it changes the marginal CV on Vc (which the paper does not report). -
No covariates: the Schoemaker 1996 paper does not
test or report any covariate effects on the LMWH PK parameters.
covariateDatais empty in both model files; downstream users wishing to add allometric scaling on weight would need to extend the model file. - No NCA comparison table: Schoemaker 1996 does not publish Cmax / Tmax / AUC / half-life NCA values for either Clexane or Fragmin. The closest reference value is the Stiekema 1993 dose-by-AUC clearance estimate of 26.7 mL/min for Clexane (vs the packaged enoxaparine model’s typical CL of 32.9 mL/min); the difference is attributed by the Schoemaker authors to the area Solution 1 attributes to the (absent in Solution 2) second compartment.
-
APTT as PD output: Schoemaker 1996 implemented
Equation 10 with the empirical-Bayes anti-Xa estimates supplied to
NONMEM as covariates driving APTT, not as a joint two-output likelihood.
The packaged
nlmixr2libmodel uses the model-predictedCc(state-derived) as the input to the exponential APTT predictor, which is the natural nlmixr2 / rxode2 two-output formulation. For typical-value forward simulation the two encodings agree; for VPC or re-fitting the small difference between empirical-Bayes Xa and model-predicted Xa as the PD driver is not reproduced. -
Example 1 not packaged: the rising-dose
anti-hypertensive example (Table 1) uses an unnamed drug and therefore
cannot be packaged as a drug-specific model under
inst/modeldb/specificDrugs/. Its parameters (t1/2_alpha = 4.80 min, t1/2_beta = 362 min, Vc = 32.7 L, CL = 155 mL/min, CV_residual = 23.1%) are recorded here for completeness only; they are not loadable throughreadModelDb().