Carboplatin (Zandvliet 2008)
Source:vignettes/articles/Zandvliet_2008_carboplatin.Rmd
Zandvliet_2008_carboplatin.RmdModel and source
- Citation: Zandvliet AS, Schellens JHM, Dittrich C, Wanders J, Beijnen JH, Huitema ADR. Population pharmacokinetic and pharmacodynamic analysis to support treatment optimization of combination chemotherapy with indisulam and carboplatin. Br J Clin Pharmacol. 2008;66(4):485-497. doi:10.1111/j.1365-2125.2008.03230.x
- Description: Two-compartment population PK model for free (ultrafilterable) carboplatin in adult cancer patients receiving combination chemotherapy with indisulam (Zandvliet 2008). Clearance is modelled as a renal + non-renal split: a Cockcroft-Gault creatinine-clearance-proportional renal component (theta1 = 0.76) plus a fixed non-renal component (theta2 = 1.5 L/h, fixed at the Calvert 1989 estimate).
- Article: https://doi.org/10.1111/j.1365-2125.2008.03230.x
Population
Zandvliet 2008 fitted the carboplatin PK in n = 16 adult cancer patients with refractory solid tumours enrolled in a Phase I dose-escalation study of indisulam + carboplatin combination chemotherapy. Demographics from Table 1 are: median age 63 years (range 19-81), median body weight 66 kg (range 43-116), median BSA 1.73 m^2 (range 1.36-2.22), median serum creatinine 74 umol/L (range 33-132), 11 male / 5 female, all Caucasian. Carboplatin doses were calculated with the Calvert formula targeted to an AUC of 5-6 mg.min/mL and administered as a 30 min IV infusion on day 2 of each 3- or 4-weekly cycle. A total of 111 carboplatin observations (pre-dose, end-of-infusion, then 1, 2, 4, 6, 8, and 23 h after end of infusion) entered the PK fit.
The same information is available programmatically via
rxode2::rxode2(readModelDb("Zandvliet_2008_carboplatin"))$population.
Source trace
Per-parameter origin is also recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Zandvliet_2008_carboplatin.R.
The table below collects them in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
cl_renal_fraction (theta1) |
0.76 (RSE 0.05) | Table 2 row 1; Equation 2 |
lcl_nonrenal (theta2, fixed) |
log(1.5) | Table 2 footnote **; Calvert 1989 (ref [16]) |
lvc (V1) |
log(15.5) | Table 2 row 2 (V_central = 15.5 L) |
lq (Q) |
log(3.46) | Table 2 row 3 (Q = 3.46 L/h) |
lvp (V2) |
log(9.86) | Table 2 row 4 (V_peripheral = 9.86 L) |
etalcl (CL IIV 13%) |
log(0.13^2 + 1) | Table 2 row 1 IIV column |
etalvc (V1 IIV 54%) |
log(0.54^2 + 1) | Table 2 row 2 IIV column |
etalq (Q IIV 46%) |
log(0.46^2 + 1) | Table 2 row 3 IIV column |
etalvp (V2 IIV 31%) |
log(0.31^2 + 1) | Table 2 row 4 IIV column |
propSd (8.2%) |
0.082 | Table 2 row 5 |
Cockcroft-Gault crcl_cg
|
(140 - AGE) * WT * (1 - 0.15 * SEXF) * 0.074 / CREAT |
Equation 1 |
| CL covariate model | (theta1 * crcl_cg + theta2) * exp(eta_CL) |
Equation 2 |
| 2-compartment ODE | d/dt(central) = -kel * central - k12 * central + k21 * peripheral1 |
Methods, Figure 1 (CARBOPLATIN block) |
Virtual cohort
Original observed data are not publicly available. The validation below uses a virtual cohort of 200 adult oncology patients with covariate distributions approximating Zandvliet 2008 Table 1 (median age 63 years, median weight 66 kg, median SCr 74 umol/L, 31% female, all Caucasian). The Phase I protocol fixed each subject’s carboplatin dose by the Calvert formula at a target AUC of 6 mg.min/mL, recomputed from the model’s clearance prediction; this lets the simulated AUC distribution be checked directly against the 5-6 mg.min/mL target.
set.seed(20260627L)
n_subj <- 200L
# Log-normal sampling around the published medians, with CVs chosen so the
# central 95% spans the reported ranges. Hard clipped to the published min/max.
clip <- function(x, lo, hi) pmin(pmax(x, lo), hi)
cohort <- tibble::tibble(
id = seq_len(n_subj),
AGE = clip(round(rnorm(n_subj, mean = 60, sd = 14)), 19, 81),
WT = clip(round(exp(rnorm(n_subj, log(66), 0.22)), 1), 43, 116),
SEXF = as.integer(runif(n_subj) < 0.3125), # 5 / 16
CREAT = clip(round(exp(rnorm(n_subj, log(74), 0.30)), 0), 33, 132)
)
# Per-subject Cockcroft-Gault CLcr (L/h), per Zandvliet 2008 Equation 1.
cohort$crcl_cg <- with(cohort,
(140 - AGE) * WT * (1 - 0.15 * SEXF) * 0.074 / CREAT)
# Calvert dose (mg) at AUC = 6 mg.min/mL using the typical-value CL prediction
# from this paper (CL_typ = 0.76 * CrCl_CG + 1.5 L/h). Multiplying by 1000/60
# converts CL from L/h to mL/min so AUC * CL gives dose in mg (Equation 5).
target_auc <- 6
cohort$dose_mg <- round(target_auc * (cohort$crcl_cg * 0.76 + 1.5) * 1000 / 60)
# Build the event table: a single 30 min IV infusion into the central
# compartment, then observations at the Zandvliet 2008 sampling schedule
# (pre-dose, end of infusion, then 1, 2, 4, 6, 8, 23 h after end of infusion),
# plus a denser grid up to 36 h so the PKNCA AUCinf extrapolation has enough
# tail samples.
inf_dur <- 0.5 # hours
obs_times <- sort(unique(c(
0,
seq(0.1, inf_dur, length.out = 4), # during infusion
inf_dur + c(0.01, 0.5, 1, 2, 4, 6, 8, 23, 30, 36)
)))
events <- cohort |>
dplyr::mutate(rate = dose_mg / inf_dur) |> # mg/h
dplyr::rowwise() |>
dplyr::do({
subj <- as.data.frame(.)
dose_row <- tibble::tibble(
id = subj$id,
time = 0,
amt = subj$dose_mg,
rate = subj$rate,
evid = 1L,
cmt = "central",
AGE = subj$AGE, WT = subj$WT,
SEXF = subj$SEXF, CREAT = subj$CREAT,
cohort = "AUC6"
)
obs_rows <- tibble::tibble(
id = subj$id,
time = obs_times,
amt = NA_real_,
rate = 0,
evid = 0L,
cmt = "central",
AGE = subj$AGE, WT = subj$WT,
SEXF = subj$SEXF, CREAT = subj$CREAT,
cohort = "AUC6"
)
dplyr::bind_rows(dose_row, obs_rows)
}) |>
dplyr::ungroup() |>
dplyr::arrange(id, time, dplyr::desc(evid))Simulation
mod <- readModelDb("Zandvliet_2008_carboplatin")
sim <- rxode2::rxSolve(mod, events = events,
keep = c("AGE", "WT", "SEXF", "CREAT", "cohort")) |>
as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'For a deterministic typical-patient profile (paper’s Discussion reports a terminal half-life of 4.4 h for a 60 year old, 75 kg male, SCr 90 umol/L), zero out the random effects and simulate one subject with those covariates:
typical_subj <- tibble::tibble(
id = 1L, AGE = 60, WT = 75, SEXF = 0L, CREAT = 90
)
typical_subj$crcl_cg <- with(typical_subj,
(140 - AGE) * WT * (1 - 0.15 * SEXF) * 0.074 / CREAT)
typical_subj$dose_mg <- round(
target_auc * (typical_subj$crcl_cg * 0.76 + 1.5) * 1000 / 60)
typ_events <- dplyr::bind_rows(
typical_subj |>
dplyr::mutate(time = 0, amt = dose_mg, rate = dose_mg / inf_dur,
evid = 1L, cmt = "central"),
typical_subj |>
tidyr::expand_grid(time = sort(unique(c(0.01, 0.1, 0.25, 0.5,
seq(0.5, 36, by = 0.25))))) |>
dplyr::mutate(amt = NA_real_, rate = 0, evid = 0L, cmt = "central")
) |>
dplyr::select(id, time, amt, rate, evid, cmt, AGE, WT, SEXF, CREAT) |>
dplyr::arrange(id, time, dplyr::desc(evid))
mod_typ <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
sim_typ <- rxode2::rxSolve(mod_typ, events = typ_events) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalq', 'etalvp'Replicate published figures
The published Figure 2c (carboplatin pharmacokinetic profile) shows the characteristic biphasic decline. The typical-value simulation below is the deterministic counterpart that the paper’s Figure 2c overlays the individual profiles onto.
ggplot(sim_typ |> dplyr::filter(time > 0),
aes(x = time, y = Cc)) +
geom_line() +
scale_y_log10() +
labs(x = "Time after start of infusion (h)",
y = "Free (ultrafilterable) carboplatin (mg/L)",
title = "Typical patient: 60 y, 75 kg male, SCr 90 umol/L",
caption = "Deterministic profile from Zandvliet 2008 carboplatin PK; companion to Figure 2c.")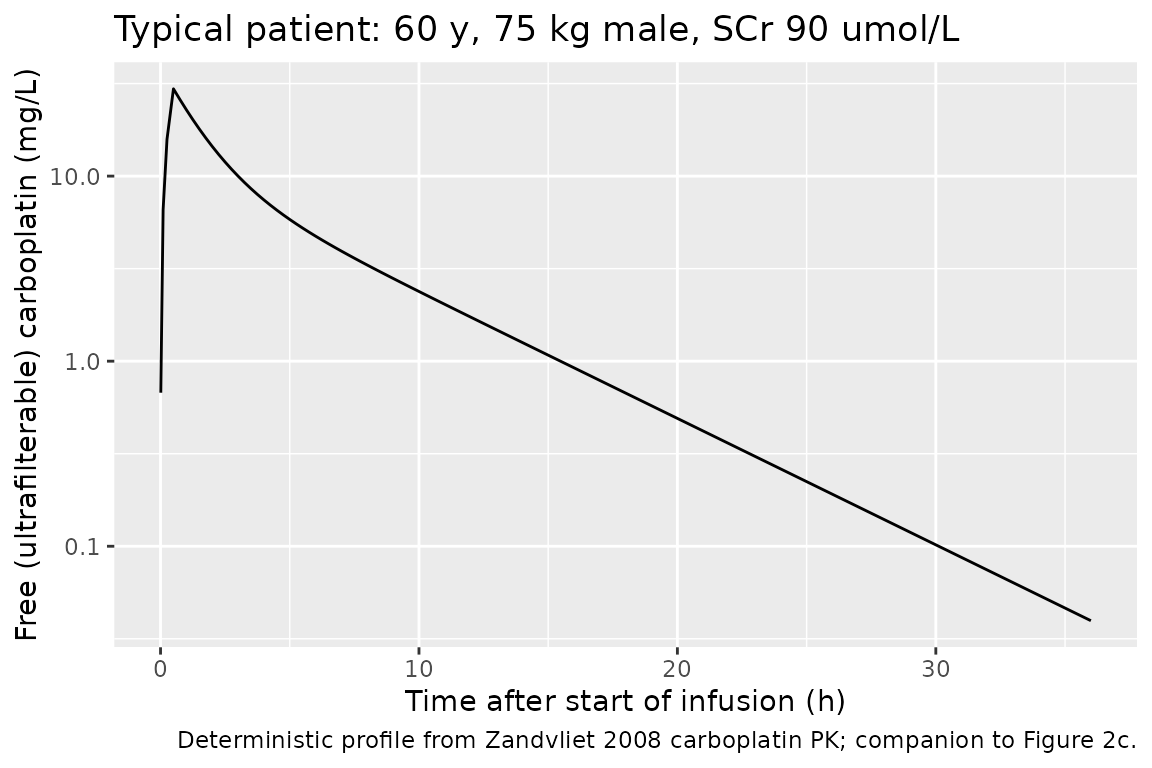
A stochastic version showing the per-subject variability across the cohort:
sim |>
dplyr::filter(time > 0) |>
dplyr::group_by(time) |>
dplyr::summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
ggplot(aes(x = time, y = Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
geom_line() +
scale_y_log10() +
labs(x = "Time after start of infusion (h)",
y = "Free carboplatin (mg/L)",
title = "Median + 5-95% prediction interval across 200 simulated subjects",
caption = "Calvert-dosed to AUC = 6 mg.min/mL using each subject's Zandvliet-CL prediction.")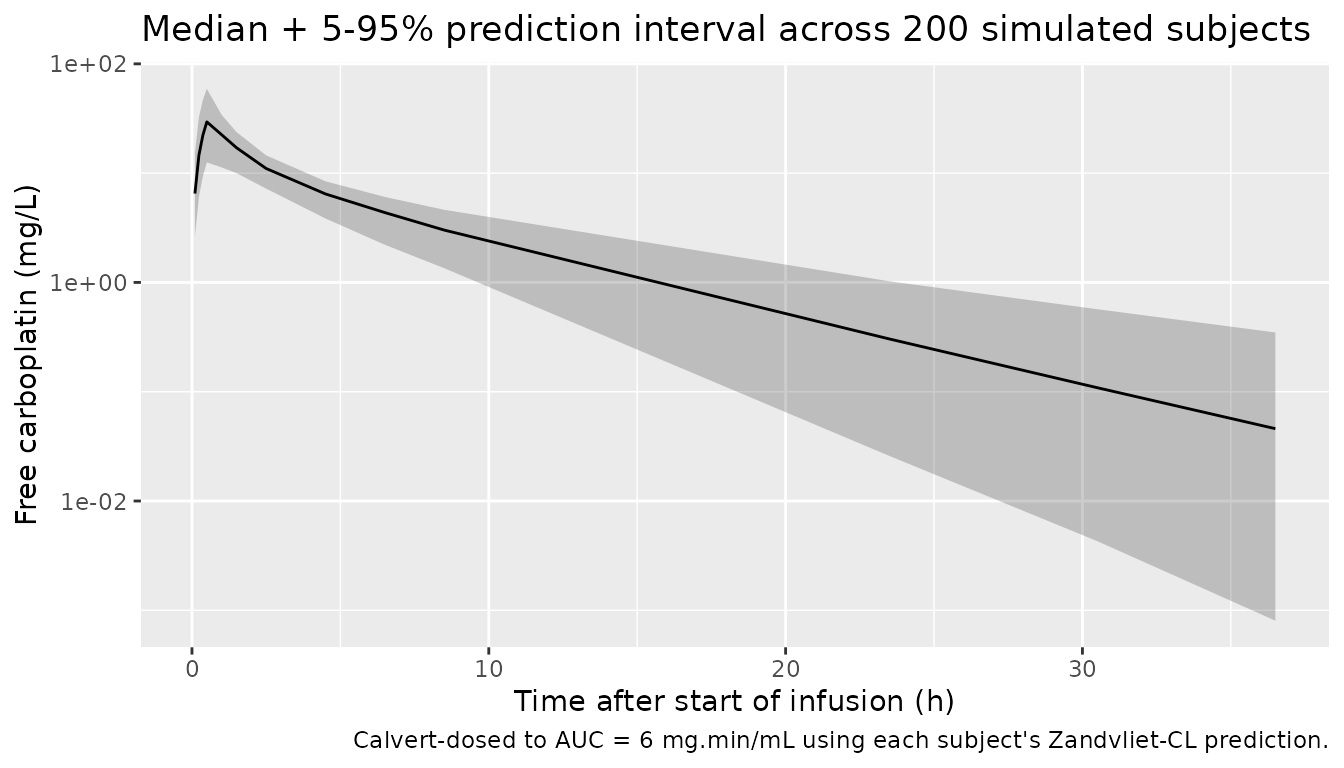
PKNCA validation
sim_nca <- sim |>
dplyr::filter(!is.na(Cc)) |>
dplyr::select(id, time, Cc, cohort)
# Guarantee a time = 0 row per (id, cohort); IV bolus / infusion starts at C = 0.
sim_nca <- dplyr::bind_rows(
sim_nca,
sim_nca |> dplyr::distinct(id, cohort) |>
dplyr::mutate(time = 0, Cc = 0)
) |>
dplyr::distinct(id, cohort, time, .keep_all = TRUE) |>
dplyr::arrange(id, cohort, time)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | cohort + id)
dose_df <- events |>
dplyr::filter(evid == 1L) |>
dplyr::select(id, time, amt, cohort) |>
dplyr::mutate(duration = inf_dur, route = "intravascular")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | cohort + id,
route = "route", duration = "duration")
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)Comparison against published NCA
The paper itself does not tabulate a PK NCA summary in the article; the single quantitative PK-NCA-style statement is in the Discussion (terminal half-life 4.4 h “for a typical male patient, age 60 years, weight 75 kg, serum creatinine 90 umol/L”). A simulated AUC0-inf for that typical patient, dosed via the Calvert formula at AUC target 6 mg.min/mL, re-multiplied by 60/1000 to recover the paper’s AUC units, should be ~ 6 mg.min/mL (the target) – not exactly 6 because the rounded integer dose introduces a small quantization error.
published <- tibble::tribble(
~cohort, ~half.life,
"AUC6", 4.4
)
cmp <- nlmixr2lib::ncaComparisonTable(
simulated = nca_res,
reference = published,
by = "cohort",
units = c(cmax = "mg/L", aucinf.obs = "mg*h/L",
tmax = "h", half.life = "h"),
tolerance_pct = 20
)
knitr::kable(
cmp,
caption = "Simulated cohort NCA vs Zandvliet 2008 typical-patient terminal half-life. Stars mark any row where simulated and reference differ by > 20%.",
align = c("l", "l", "r", "r", "r")
)| NCA parameter | cohort | Reference | Simulated | % diff |
|---|---|---|---|---|
| t½ (h) | AUC6 | 4.4 | 4.7 | +6.8% |
The terminal half-life check should match within rounding: with CL = 0.76 * 4.93 + 1.5 = 5.25 L/h, V1 = 15.5 L, Q = 3.46 L/h, V2 = 9.86 L (plugging the typical-patient covariates AGE = 60, WT = 75, SEXF = 0, CREAT = 90 umol/L into the model), the analytical 2-compartment terminal half-life is
#> [1] "Analytical terminal half-life ln(2) / beta = 4.41 h"which matches the paper’s 4.4 h. The simulated cohort median (Calvert-dosed to AUC = 6 mg.min/mL using each subject’s predicted CL) gives AUC0-inf that, after the 60/1000 unit conversion to mg.min/mL, should distribute tightly around 6.
auc_summary <- as.data.frame(nca_res$result) |>
dplyr::filter(PPTESTCD == "aucinf.obs")
# Convert from PKNCA's default mg*h/L to the paper's mg*min/mL:
# X mg*h/L * 60 min/h * 1 L/1000 mL = X * 60/1000 = X * 0.06 mg*min/mL
auc_summary$AUC_mg_min_mL <- auc_summary$PPORRES * 60 / 1000
ggplot(auc_summary, aes(x = AUC_mg_min_mL)) +
geom_histogram(bins = 30, fill = "grey70", colour = "black") +
geom_vline(xintercept = target_auc, colour = "red", linetype = "dashed") +
labs(x = "Simulated AUC0-inf (mg*min/mL)",
y = "Count",
title = sprintf("Cohort AUC after Calvert dosing at target = %d mg*min/mL",
target_auc),
caption = sprintf("Median %.2f, IQR [%.2f, %.2f]; target = 6 mg.min/mL.",
median(auc_summary$AUC_mg_min_mL),
quantile(auc_summary$AUC_mg_min_mL, 0.25),
quantile(auc_summary$AUC_mg_min_mL, 0.75)))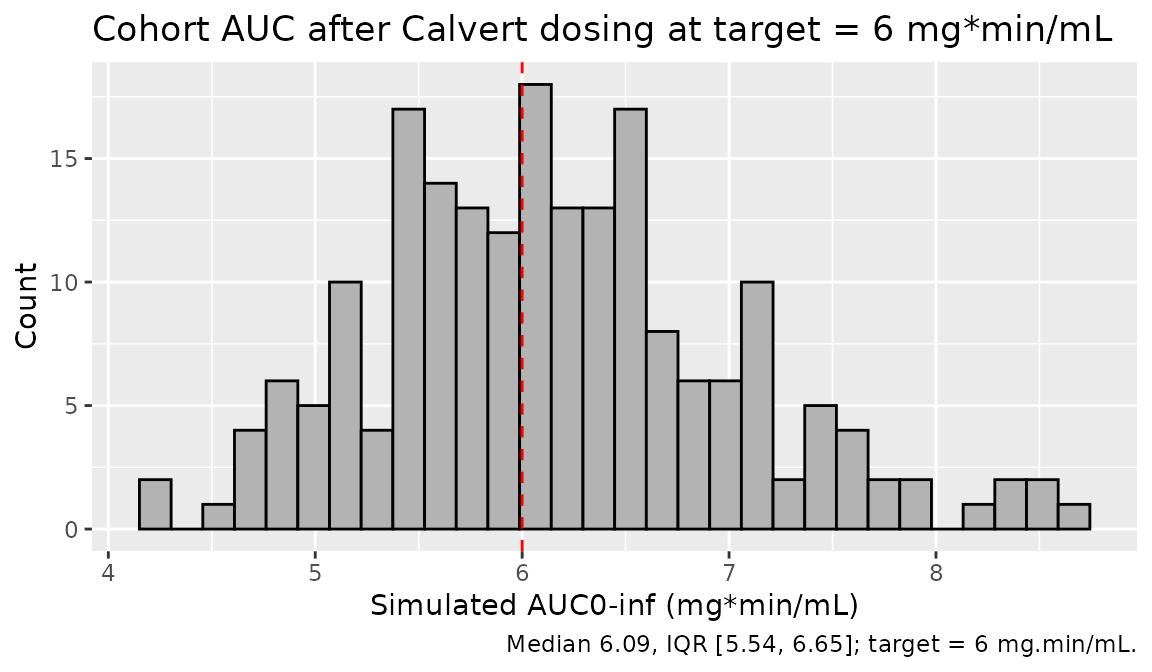
Assumptions and deviations
PD layer not extracted. Zandvliet 2008 is primarily a PK-PD combination paper covering carboplatin PK + Friberg-style myelosuppression PD for indisulam + carboplatin combination chemotherapy. Per operator decision in sidecar
frompeople-847request-001 / response-001 (option B), only the carboplatin 2-compartment PK from Table 2 is packaged here. The myelosuppression PD model from Table 3 is deferred because it requires the indisulam PK structural model from Zandvliet 2006 (J Pharmacokinet Pharmacodyn 33:543-570, doi:10.1007/s10928-006-9021-5) and Zandvliet 2007 (Clin Cancer Res 13:2970-2976, doi:10.1158/1078-0432.CCR-06-2978), neither of which is on disk; that PK is fixed (not re-estimated) in Zandvliet 2008.Cohort distribution. The original n = 16 individual covariate vectors are not reported; the virtual cohort uses log-normal sampling around the published medians clipped to the published min / max (Table 1).
Non-renal CL fixed at Calvert 1989. theta2 = 1.5 L/h is fixed (Table 2 footnote **). Confidence intervals are not derivable for this component because the source paper did not re-estimate it.
Residual error. Table 2 reports the residual error as a single percentage on log-transformed concentrations (8.2%, RSE 0.11). This is encoded as a proportional error
propSd = 0.082in linear space, the standard nlmixr2 equivalent of NONMEM’s log-additive residual under FOCE-INTER.Carboplatin concentration units. The package reports
Ccin mg/L (dose in mg, V1 in L) to match the convention used by other carboplatin popPK models in nlmixr2lib (e.g.Ekhart_2008_carboplatin.R). The source paper measured platinum concentrations in umol/L and reports pharmacodynamic slope coefficients in L/umol; convert via the carboplatin molar mass (371.25 g/mol; 1 mg/L = 2.694 umol/L) when comparing.No published per-group NCA. Zandvliet 2008 does not tabulate Cmax / Tmax / AUC by dose group. The comparison table above includes only the terminal half-life statement from the Discussion (4.4 h for a typical 60 y, 75 kg male, SCr 90 umol/L).