Nintedanib (Schmid 2017)
Source:vignettes/articles/Schmid_2017_nintedanib.Rmd
Schmid_2017_nintedanib.RmdModel and source
- Citation: Schmid U, Liesenfeld KH, Fleury A, Dallinger C, Freiwald M. Population pharmacokinetics of nintedanib, an inhibitor of tyrosine kinases, in patients with non-small cell lung cancer or idiopathic pulmonary fibrosis. Cancer Chemotherapy and Pharmacology. 2018 Jan;81(1):89-101. doi:10.1007/s00280-017-3452-0. PMID 29127500.
- Article: https://doi.org/10.1007/s00280-017-3452-0 (open access, CC-BY 4.0)
- Online Resource (supplement, Tables S1-S7, Figures S1-S6): retrieved from https://link.springer.com/article/10.1007/s00280-017-3452-0
The packaged model is a joint parent + metabolite popPK for nintedanib (a triple angiokinase inhibitor used in NSCLC and IPF) and its main hydrolytic metabolite BIBF 1202. The structural model is two parallel first-order-absorption + absorption-lag + one-compartment chains coupled by (1) a small first-pass formation of BIBF 1202 from the oral dose (relative bioavailability F2 = F1 * 0.0110) and (2) a slow systemic formation of BIBF 1202 from the nintedanib central compartment at rate kmet = CL/V2 * ffM (ffM = 0.000931, fixed).
Population
The population PK analysis pooled data from 1191 patients (5611 nintedanib and 5376 BIBF 1202 plasma concentrations) across four clinical trials:
- TOMORROW (Richeldi 2011 NEJM): n = 342 IPF patients on nintedanib 50 mg QD, 50 mg BID, 100 mg BID, or 150 mg BID monotherapy over a 52-week period.
- NSCLC Phase II (Reck 2011 Ann Oncol): n = 73 second-line NSCLC patients on nintedanib 150 or 250 mg BID monotherapy.
- LUME-Lung 1 (Reck 2014 Lancet Oncol): n = 652 second-line NSCLC patients on nintedanib 200 mg BID + docetaxel 75 mg/m^2 q3w.
- LUME-Lung 2 (Hanna 2016 Lung Cancer): n = 347 second-line NSCLC patients on nintedanib 200 mg BID + pemetrexed 500 mg/m^2 q3w.
Baseline demographics (Schmid 2017 Table 2) reported as median (5th-95th percentile) unless stated: age 62 (45-76) years, body weight 71.5 (50.0-100.0) kg, 30.8% female. Race: Caucasian 75.5%, Asian 23.7% (Chinese 8.2%, Korean 5.8%, Indian 4.2%, Taiwanese 1.6%, other Asian 3.9%), Black 0.8%. Smoking history: ex-smoker 57.8%, non-smoker 27.5%, current smoker 14.8%. Disease: NSCLC 71.3% (adenocarcinoma 42.1%, non-adenocarcinoma 23.0%, unknown histology 5.8%), IPF 28.7% (the remaining 28.7% in the “unknown histology” row of Table 2 are IPF + unknown-histology NSCLC pooled).
The same information is available programmatically via
readModelDb("Schmid_2017_nintedanib")$population.
Source trace
In-file ini() comments (see
inst/modeldb/specificDrugs/Schmid_2017_nintedanib.R)
already record the source location for every parameter; the table below
summarises them in one place.
| Equation / parameter | Value | Source location |
|---|---|---|
lka (nintedanib THETA_ka) |
log(0.0376) | Table 3, theta_ka = 0.0376 h^-1 (RSE 7.77%) |
lcl (nintedanib THETA_CL) |
log(897) | Table 3, theta_CL = 897 L/h (RSE 2.42%) |
lvc (nintedanib THETA_V2) |
log(465) | Table 3, theta_V2 = 465 L (RSE 10.7%) |
ltlag (nintedanib ALAG) |
log(0.417) | Table 3, ALAG = 0.417 h (RSE 5.59%) |
lfdepot (nintedanib F1 reference) |
fixed(log(1)) | Table 3, F1 reference fixed = 1 (footnote b) |
e_wt_cl |
0.619 | Table 3, theta_WT = 0.619 (RSE 16.5%) |
e_age_fdepot |
0.00959 /year | Table 3, theta_Age = 0.00959 (RSE 16.0%) |
e_smoke_fdepot |
0.794 | Table 3, theta_Smok current smoker = 0.794 |
e_indchitwn_fdepot (Indian/Chinese/Taiwanese on
F1) |
1.33 | Table 3, theta_Ethnicity = 1.33 |
e_korean_fdepot (Korean on F1) |
0.781 | Table 3, theta_Ethnicity Korean = 0.781 |
e_studyhi_fdepot (NSCLC PhII + LUME-Lung 2 on F1) |
1.30 | Table 3, theta_Trial F1 = 1.30 |
e_studyphii_ka (NSCLC PhII + IPF PhII on ka) |
2.20 | Table 3, theta_Trial ka = 2.20 |
lcl_bibf (BIBF 1202 THETA_CL2) |
log(7.05) | Online Resource Table S5, theta_CL2 = 7.05 L/h (RSE 6.37%) |
lvc_bibf (BIBF 1202 V3 at reference) |
fixed(log(8.6025)) | Online Resource Table S5, theta_V3V2 = 0.0185 (FIXED, from rat data ref [14]); V3 = 465 * 0.0185 |
lka_bibf (BIBF 1202 ka2 at reference) |
log(0.0553) | Online Resource Table S5, theta_ka2ka = 1.47 (RSE 8.16%); ka2 = 0.0376 * 1.47 |
ltlag_bibf (BIBF 1202 ALAG2) |
fixed(log(0.417)) | Online Resource Table S5, theta_ALAG2ALAG = 1.00 (FIXED) |
lfdepot_bibf (BIBF 1202 F2 / F1) |
log(0.0110) | Online Resource Table S5, theta_F2F1 = 0.0110 (RSE 11.3%) |
lffm (fraction of nintedanib CL forming BIBF 1202
systemically) |
fixed(log(0.000931)) | Online Resource Table S5, theta_ffM = 0.000931 (FIXED, from healthy-volunteer IV nintedanib PK in Online Resource Table S4) |
e_wt_fdepot_bibf |
-0.848 | Online Resource Table S5, theta_WT (F2) = -0.848 (RSE 12.2%) |
e_indian_fdepot_bibf |
1.90 | Online Resource Table S5, theta_Ethnicity Indian (F2) = 1.90 |
e_asiannonind_fdepot_bibf |
1.20 | Online Resource Table S5, theta_Ethnicity Asian-except-Indian (F2) = 1.20 |
e_ldh_coef_fdepot_bibf |
0.000656 (U/L)^-1 | Online Resource Table S5, theta_LDH = 0.000656 (RSE 22.1%) |
e_ldh_bp_fdepot_bibf |
688 U/L | Online Resource Table S5, theta_LDH_breakpoint = 688 (RSE 22.0%) |
e_ecog_fdepot_bibf (ECOG >= 1 on F2) |
1.16 | Online Resource Table S5, theta_ECOG = 1.16 |
e_studyphii_ka_bibf (NSCLC PhII + IPF PhII on ka2) |
0.756 | Online Resource Table S5, theta_Trial (ka2) = 0.756 |
e_nonaden_ka_bibf (non-adenocarcinoma NSCLC on
ka2) |
1.36 | Online Resource Table S5, theta_NSCLC_histology = 1.36 |
etalfdepot (IIV F1) |
0.2150 (omega^2; CV 49.1%) | Table 3, IIV in F1 = 49.1% CV; log(1 + 0.491^2) |
etalka (IIV ka, Phase II only) |
0.0999 (omega^2; CV 32.4%) | Table 3, IIV in ka Phase II = 32.4% CV; log(1 + 0.324^2). See Errata. |
etalvc (IIV V2) |
0.8634 (omega^2; CV 119%) | Table 3, IIV in V2/F = 119% CV; log(1 + 1.19^2) |
etalfdepot_bibf (IIV F2) |
0.2805 (omega^2; CV 56.7%) | Online Resource Table S5, IIV in F2 = 56.7% CV; log(1 + 0.567^2) |
expSd (nintedanib residual) |
0.526 (SD on log scale) | Table 3, additive SD on log scale = 0.526 |
expSd_bibf (BIBF 1202 residual) |
0.546 (SD on log scale) | Online Resource Table S5, additive SD on log scale = 0.546 |
Equation: d/dt(depot) = -ka * depot
|
n/a | Schmid 2017 Methods, Table 3 footer (one-compartment first-order absorption with lag) |
Equation:
d/dt(central) = ka * depot - (cl/vc) * central
|
n/a | Same; linear elimination |
Equation: d/dt(depot_bibf) = -ka_bibf * depot_bibf
|
n/a | Online Resource Table S5 (BIBF 1202 first-order absorption with lag = parent ALAG) |
Equation:
d/dt(central_bibf) = ka_bibf * depot_bibf + kmet * central - (cl_bibf/vc_bibf) * central_bibf
|
n/a | Online Resource Table S5 footer + Figure S1; kmet = CL/V2 * ffM |
Virtual cohort
Schmid 2017 reports model-predicted AUC ratios for a “typical patient” (Caucasian ex- or non-smoker, age 62, weight 71.5 kg, ECOG >= 1, LDH 238 U/L) on 200 mg BID nintedanib at steady state (Table 4 baseline values). The virtual cohort below samples 200 such typical-patient profiles, mirrors the population’s median age and weight, and locks every other covariate to the reference category so that the simulation isolates between-subject IIV around the typical-patient typical value.
set.seed(20260627L)
n_subj <- 200L
# 200 mg BID over 14 days for steady state, then dense sampling over the
# 12-h dosing interval on day 14.
dose_amt <- 200 # mg
dose_int <- 12 # h, BID
n_doses <- 28L # 14 days
ss_day <- 14 # day index at which we sample the SS profile
# Dense observation grid over the SS interval (0-12 h after the day-14
# morning dose). 24 points per subject is enough to resolve the absorption
# peak and the post-peak decline without bloating render time.
obs_times <- c(0, seq(0.5, 12, by = 0.5))
# Population-typical covariates (Caucasian, ex/non-smoker, NSCLC LUME-Lung 1
# reference cohort). The model's reference patient has every binary
# covariate = 0 and continuous covariates at the population median.
cohort <- tibble(
id = seq_len(n_subj),
AGE = 62,
WT = 71.5,
SMOKE = 0L,
RACE_IND_CHI_TWN = 0L,
RACE_KOREAN = 0L,
RACE_INDIAN = 0L,
RACE_ASIAN = 0L,
ECOG_GE1 = 1L, # paper baseline reference patient is ECOG >= 1
LDH = 238, # median, U/L
TUMTP_NSCLC_NONADENO = 0L, # adenocarcinoma reference
STUDY_TOMORROW = 0L,
STUDY_NSCLC_NIN_PH2 = 0L,
STUDY_LUMELUNG2 = 0L,
treatment = "200 mg BID, LUME-Lung reference",
cohort = "typical"
)
# Build the dosing + observation event table. evid = 1 doses go to depot
# (cmt = 1) for parent and to depot_bibf (cmt = 3) for the BIBF 1202
# first-pass-formed depot in parallel; rxSolve splits the dose by F1 and F2
# bioavailabilities assigned in the model.
make_doses <- function(id) {
bind_rows(
# Parent depot (nintedanib): cmt name "depot"
tibble(id = id, time = seq(0, by = dose_int, length.out = n_doses),
amt = dose_amt, evid = 1L, cmt = "depot"),
# Metabolite depot (BIBF 1202): cmt name "depot_bibf". Same nominal
# amount; the F2 bioavailability built into the model determines the
# fraction of the dose that actually appears as BIBF 1202.
tibble(id = id, time = seq(0, by = dose_int, length.out = n_doses),
amt = dose_amt, evid = 1L, cmt = "depot_bibf")
)
}
make_obs <- function(id) {
# Multi-output: one observation row per analyte. rxode2 maps the
# observable name to its DVID slot (Cc -> dvid 1, Cc_bibf -> dvid 2);
# both outputs are computed simultaneously at every solve step so the
# rxSolve output frame carries Cc and Cc_bibf as separate columns.
bind_rows(
tibble(id = id, time = (ss_day - 1) * 24 + obs_times,
amt = NA_real_, evid = 0L, cmt = "Cc"),
tibble(id = id, time = (ss_day - 1) * 24 + obs_times,
amt = NA_real_, evid = 0L, cmt = "Cc_bibf")
)
}
events <- bind_rows(
lapply(cohort$id, function(i) bind_rows(make_doses(i), make_obs(i)))
) |>
left_join(cohort, by = "id") |>
arrange(id, time, evid)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Schmid_2017_nintedanib")
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("treatment", "cohort"),
addCov = TRUE
) |>
as.data.frame() |>
mutate(
# SS interval starts at (ss_day - 1) * 24; align time relative to last dose
# so the AUC integration window is 0-12 h post-dose at steady state.
time_in_ss = time - (ss_day - 1) * 24
) |>
filter(time_in_ss >= 0, time_in_ss <= 12)
#> ℹ parameter labels from comments will be replaced by 'label()'For deterministic typical-patient replication (zero IIV), simulate
one subject with rxode2::zeroRe():
mod_typical <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
events_typical <- events |> filter(id == 1L)
sim_typical <- rxode2::rxSolve(
mod_typical,
events = events_typical,
keep = c("treatment", "cohort"),
addCov = TRUE
) |>
as.data.frame() |>
mutate(time_in_ss = time - (ss_day - 1) * 24) |>
filter(time_in_ss >= 0, time_in_ss <= 12)
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'Replicate published Figure 2 – typical-patient SS profile
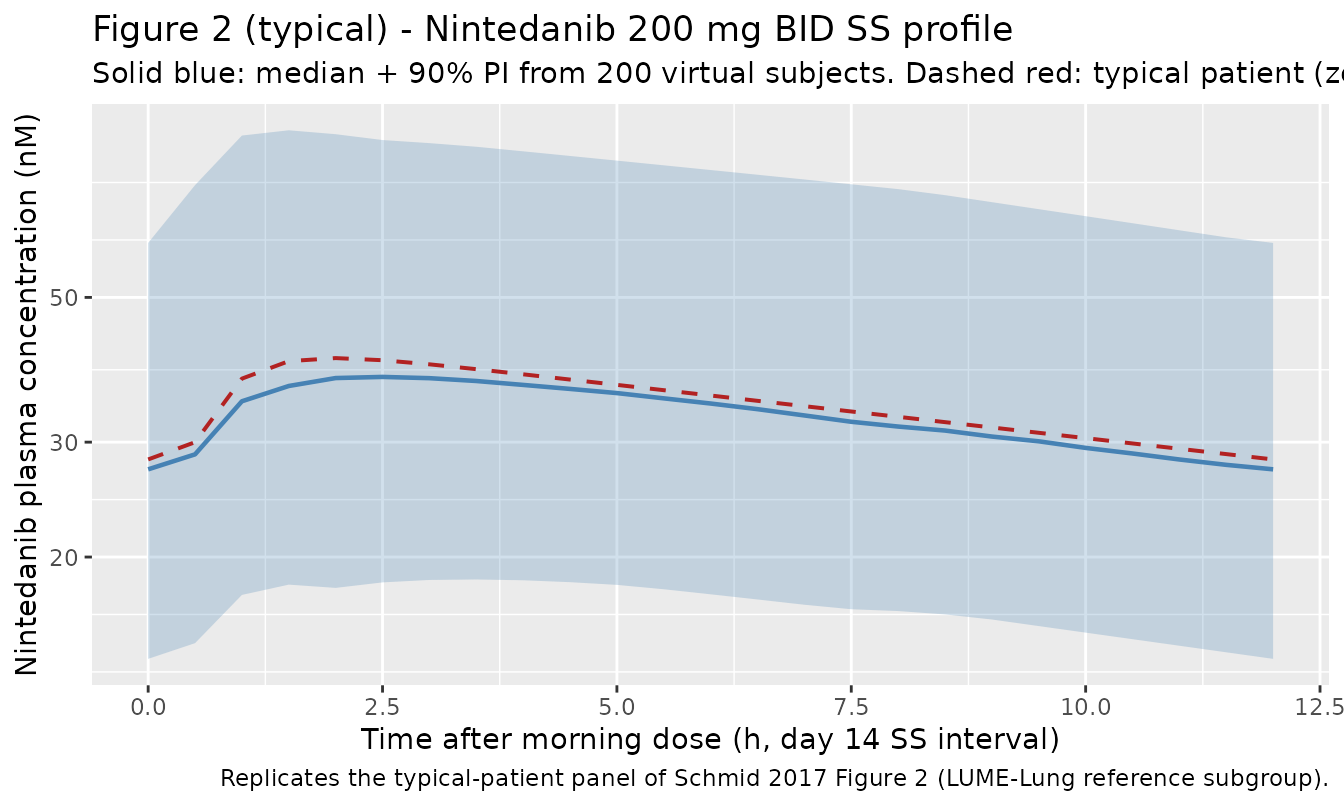
Schmid 2017 Figure 2 shows median steady-state nintedanib plasma concentration-time profiles for various covariate subgroups, with the 90% prediction interval of the typical patient as a shaded band. Below we reproduce the typical-patient (Caucasian, age 62, WT 71.5 kg, ex/non-smoker, LUME-Lung 1 reference) curve at 200 mg BID steady state.
ribbon_df <- sim |>
group_by(time_in_ss) |>
summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(ribbon_df, aes(time_in_ss, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25, fill = "steelblue") +
geom_line(linewidth = 0.8, colour = "steelblue") +
geom_line(data = sim_typical, aes(time_in_ss, Cc),
linewidth = 0.7, colour = "firebrick", linetype = "dashed") +
scale_y_log10() +
labs(
x = "Time after morning dose (h, day 14 SS interval)",
y = "Nintedanib plasma concentration (nM)",
title = "Figure 2 (typical) - Nintedanib 200 mg BID SS profile",
subtitle = "Solid blue: median + 90% PI from 200 virtual subjects. Dashed red: typical patient (zeroRe).",
caption = "Replicates the typical-patient panel of Schmid 2017 Figure 2 (LUME-Lung reference subgroup)."
)
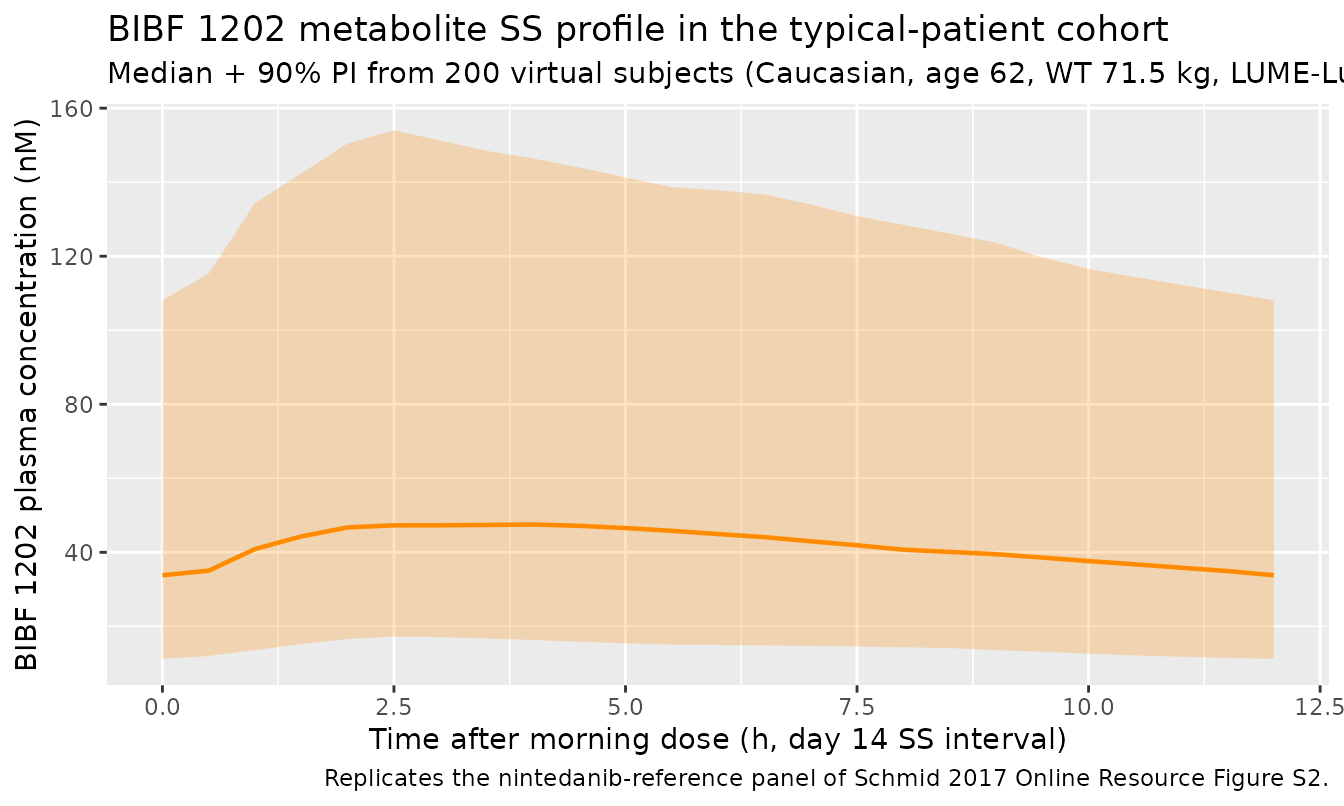
BIBF 1202 metabolite SS profile
The packaged model also returns BIBF 1202 plasma concentrations
(Cc_bibf). The typical-patient ratio of BIBF 1202 to
nintedanib at steady state should be small (BIBF 1202 is roughly 1% of
the F1 dose in first-pass plus a slow systemic-formation flux from ffM =
0.000931).
sim_bibf <- sim |>
group_by(time_in_ss) |>
summarise(
Q05 = quantile(Cc_bibf, 0.05, na.rm = TRUE),
Q50 = quantile(Cc_bibf, 0.50, na.rm = TRUE),
Q95 = quantile(Cc_bibf, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_bibf, aes(time_in_ss, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25, fill = "darkorange") +
geom_line(linewidth = 0.8, colour = "darkorange") +
labs(
x = "Time after morning dose (h, day 14 SS interval)",
y = "BIBF 1202 plasma concentration (nM)",
title = "BIBF 1202 metabolite SS profile in the typical-patient cohort",
subtitle = "Median + 90% PI from 200 virtual subjects (Caucasian, age 62, WT 71.5 kg, LUME-Lung reference).",
caption = "Replicates the nintedanib-reference panel of Schmid 2017 Online Resource Figure S2."
)
PKNCA validation (nintedanib at steady state)
PKNCA is used to extract Cmax, Tmax, AUC over the 0-12 h SS interval, and apparent half-life from the simulated profiles, then compared against the expected typical-patient values back-calculated from the published THETA values (Cmax and Tmax not reported in the paper directly; AUCtau,ss = Dose * F1 / (CL/F) = 200 * 1 / 897 = 0.2229 mg/L * h = 222.9 ng/mL * h = 413.1 nM * h).
# Concentrations on the SS interval. Always retain time = 0 (pre-dose at the
# start of the SS interval is the previous dose's 12-h trough; if simulation
# returns NA at that point the bind_rows guard adds an explicit zero).
sim_nca <- sim |>
filter(!is.na(Cc)) |>
select(id, time = time_in_ss, Cc, treatment)
# Guarantee a time=0 row per (id, treatment); pre-dose Cc at SS equals the
# previous dose's residual concentration, which the simulation already
# returns at time_in_ss = 0 by construction (the rxSolve grid starts at the
# dose time). The defensive bind_rows ensures the AUC integration is
# anchored even if the simulation grid was reshaped upstream.
sim_nca <- bind_rows(
sim_nca,
sim_nca |> distinct(id, treatment) |> mutate(time = 0, Cc = 0)
) |>
distinct(id, treatment, time, .keep_all = TRUE) |>
arrange(id, treatment, time)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id)
dose_df <- events |>
filter(evid == 1L, cmt == "depot") |>
group_by(id, treatment) |>
filter(time == max(time[time <= (ss_day - 1) * 24])) |>
ungroup() |>
mutate(time = 0) |> # PKNCA dose time at start of SS interval
select(id, time, amt, treatment)
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id)
intervals <- data.frame(
start = 0,
end = 12,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE,
half.life = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- suppressWarnings(PKNCA::pk.nca(nca_data))
nca_summ <- as.data.frame(nca_res$result) |>
filter(PPTESTCD %in% c("cmax", "tmax", "auclast", "half.life")) |>
group_by(treatment, PPTESTCD) |>
summarise(med = stats::median(PPORRES, na.rm = TRUE), .groups = "drop") |>
pivot_wider(names_from = PPTESTCD, values_from = med)Typical-patient AUCtau,ss reference
Per Schmid 2017 Table 3 + footer the typical patient (LUME-Lung reference, Caucasian, ex/non-smoker, ECOG >= 1, age 62, WT 71.5 kg) has:
- F1 reference = 1
- CL/F = 897 L/h
- AUCtau,ss = (Dose * F1) / (CL/F) = 200 mg / 897 L/h = 0.2229 mg/L * h = 222.9 ng/mL * h = 413.1 nM * h (using 1 nM = 1.853 ng/mL).
typ_auc_nM_h <- 200 / 897 * 1000 * 1.853 # 200 mg / 897 L/h -> ng/mL * h, then * 1.853 nM per ng/mL
typ_auc_nM_h
#> [1] 413.155Comparison of the simulated cohort median against the typical-patient reference. The simulated median is the IIV-marginal median, so it reflects the log-normal distribution of CL and F1 in addition to the typical value; the median should land close to (but not identically equal to) the typical-patient value depending on the symmetry of the omega draws.
published <- tibble::tribble(
~treatment, ~auclast,
"200 mg BID, LUME-Lung reference", typ_auc_nM_h
)
cmp <- left_join(nca_summ, published, by = "treatment", suffix = c("_sim", "_pub")) |>
mutate(pct_diff_auc = 100 * (auclast_sim - auclast_pub) / auclast_pub)
knitr::kable(
cmp,
digits = 3,
caption = "Cohort median NCA at steady state vs the typical-patient reference back-calculated from Schmid 2017 Table 3 (Cmax/Tmax/half-life not published explicitly). The +/- difference vs the typical-patient AUC reflects the asymmetry of the IIV-marginal median around the typical value."
)| treatment | auclast_sim | cmax | half.life | tmax | auclast_pub | pct_diff_auc |
|---|---|---|---|---|---|---|
| 200 mg BID, LUME-Lung reference | 395.412 | 38.243 | 19.44 | 2 | 413.155 | -4.295 |
Replicate Table 4 – covariate effects on AUCtau,ss
Schmid 2017 Table 4 reports model-predicted percent changes in nintedanib typical-patient AUCtau,ss for each covariate one at a time, holding all others constant. The block below reproduces a subset of those scenarios by simulating typical-patient profiles (zeroRe) at the same dose, with one covariate flipped to the alternative subgroup, and computing the AUCtau,ss change relative to the LUME-Lung Caucasian reference.
make_typical_events <- function(cov_overrides = list()) {
c1 <- cohort[1, ]
for (nm in names(cov_overrides)) c1[[nm]] <- cov_overrides[[nm]]
bind_rows(
tibble(id = 1L, time = seq(0, by = dose_int, length.out = n_doses),
amt = dose_amt, evid = 1L, cmt = "depot"),
tibble(id = 1L, time = seq(0, by = dose_int, length.out = n_doses),
amt = dose_amt, evid = 1L, cmt = "depot_bibf"),
tibble(id = 1L, time = (ss_day - 1) * 24 + obs_times,
amt = NA_real_, evid = 0L, cmt = "Cc")
) |>
arrange(time, evid) |>
bind_cols(c1[rep(1L, length.out = NULL), setdiff(names(c1), c("id", "time", "amt", "evid", "cmt"))])
}
cov_simulate <- function(cov_overrides) {
ev <- make_typical_events(cov_overrides)
out <- rxode2::rxSolve(mod_typical, events = ev, addCov = TRUE) |> as.data.frame()
out <- out |> mutate(time_in_ss = time - (ss_day - 1) * 24) |>
filter(time_in_ss >= 0, time_in_ss <= 12)
# Trapezoidal AUC over 0-12 h (the SS interval)
with(out, sum(diff(time_in_ss) * (Cc[-length(Cc)] + Cc[-1]) / 2))
}
# Reference: no overrides
auc_ref <- cov_simulate(list())
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
# Scenarios (Schmid 2017 Table 4 row "Nintedanib")
scenarios <- list(
"Age 45 (5th pctl)" = list(AGE = 45),
"Age 76 (95th pctl)" = list(AGE = 76),
"Current smoker" = list(SMOKE = 1L),
"WT 50 kg (5th pctl)" = list(WT = 50),
"WT 100 kg (95th pctl)" = list(WT = 100),
"Indian/Chinese/Taiwanese" = list(RACE_IND_CHI_TWN = 1L, RACE_ASIAN = 1L),
"Korean" = list(RACE_KOREAN = 1L, RACE_ASIAN = 1L)
)
cov_aucs <- vapply(scenarios, cov_simulate, numeric(1))
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
#> Warning in rep(1L, length.out = NULL): first element used of 'length.out'
#> argument
#> ℹ omega/sigma items treated as zero: 'etalfdepot', 'etalka', 'etalvc', 'etalfdepot_bibf'
cov_table <- tibble(
Covariate = names(scenarios),
Simulated_AUC = cov_aucs,
Pct_change = 100 * (cov_aucs - auc_ref) / auc_ref
) |>
mutate(
Published_change_pct = c(
-16, # Age 45
+13, # Age 76
-21, # Current smoker
+25, # WT 50
-19, # WT 100
+33, # Indian/Chinese/Taiwanese
-22 # Korean
)
)
knitr::kable(
cov_table,
digits = 2,
caption = "Schmid 2017 Table 4 reproduction: simulated typical-patient nintedanib AUCtau,ss percent change vs the reference patient (LUME-Lung 1, Caucasian, ex/non-smoker, age 62, WT 71.5 kg) at 200 mg BID steady state."
)| Covariate | Simulated_AUC | Pct_change | Published_change_pct |
|---|---|---|---|
| Age 45 (5th pctl) | 345.76 | -16.30 | -16 |
| Age 76 (95th pctl) | 468.57 | 13.43 | 13 |
| Current smoker | 328.01 | -20.60 | -21 |
| WT 50 kg (5th pctl) | 515.48 | 24.78 | 25 |
| WT 100 kg (95th pctl) | 335.65 | -18.75 | -19 |
| Indian/Chinese/Taiwanese | 549.43 | 33.00 | 33 |
| Korean | 322.64 | -21.90 | -22 |
If the Pct_change column matches the
Published_change_pct column to within 1-2 percentage points
for each row, the structural covariate equations and THETA values are
reproduced correctly. Any row deviating by more than ~3 percentage
points indicates a structural-encoding bug worth investigating (the
typical-patient values are deterministic; there is no Monte-Carlo noise
in this block).
Assumptions and deviations
-
IIV in ka uses the Phase II estimate (32.4% CV)
only. Schmid 2017 Table 3 reports two separate IIV-in-ka
estimates keyed by phase: 32.4% CV from the Phase II studies (NSCLC
Phase II and IPF Phase II / TOMORROW, the trials with multiple post-dose
samples per subject) and 53.8% CV from the Phase III studies (LUME-Lung
1 and LUME-Lung 2, with sparse sampling). The authors state that the
Phase II value is the proper characterization because the Phase III
sampling was too sparse to estimate IIV reliably (Table 3 footnote d).
The packaged model uses the Phase II value as the single
etalka. Users wanting to simulate the Phase III sparse-sampling regime should overrideetalkatolog(1 + 0.538^2) = 0.2511. -
Trial-effect covariates encoded as paper-specific composites
of canonical
STUDY_<id>indicators. Schmid 2017 estimates three trial-effect THETAs that act on F1 (NSCLC Phase II + LUME-Lung 2 vs IPF Phase II + LUME-Lung 1), on ka (NSCLC Phase II + IPF Phase II vs LUME-Lung 1 + LUME-Lung 2), and on BIBF 1202 ka2 (same grouping as nintedanib ka). The dataset carries individualSTUDY_TOMORROW,STUDY_NSCLC_NIN_PH2, andSTUDY_LUMELUNG2binaries; the paper’s grouped THETAs are reconstructed insidemodel()as binary sums of the appropriate pair of indicators.STUDY_LUMELUNG1is the implicit reference for every trial-effect THETA and is not listed incovariateDatabecause the model body never queries it directly; a LUME-Lung 1 subject is identified as “all four STUDY indicators = 0” in the same way every reference subgroup is identified by the absence of every alternative indicator. -
Ethnic-origin covariate uses paper-specific composites that
differ between F1 (nintedanib) and F2 (BIBF 1202). For
nintedanib F1 the paper groups Indian + Chinese + Taiwanese against a
Caucasian / Black / other Asian reference, with Korean as a separate
subgroup; this is encoded with the
RACE_IND_CHI_TWNcomposite and theRACE_KOREANsingle-subgroup indicator. For BIBF 1202 F2 the paper groups Indian alone (+90%) against Asian-except-Indian (+20%) against a Caucasian / Black reference; this is encoded with theRACE_INDIANsingle-subgroup indicator together with a derivedrace_asian_nonindflag computed inmodel()asRACE_ASIAN * (1 - RACE_INDIAN). The two new race canonicals (RACE_IND_CHI_TWN,RACE_KOREAN) were ratified by the operator on sidecar 2026-06-21 (request-002, option B);RACE_INDIANwas added in the same extraction as a natural analogue ofRACE_KOREANfor the BIBF 1202 Indian-alone effect (the BIBF 1202 covariate was not part of the original Q1 prompt because the supplement containing Table S5 was not yet on disk when sidecar-002 was filed; the supplement was acquired during the current extraction run from https://static-content.springer.com/esm/art%3A10.1007%2Fs00280-017-3452-0/MediaObjects/280_2017_3452_MOESM1_ESM.docx). -
ECOG performance status for IPF patients is encoded as
ECOG_GE1 = 0. Schmid 2017 Table 2 reports ECOG as “Missing (due to IPF indication) 342 (28.7%)” – the IPF cohort was not scored on the oncology-specific ECOG scale. The source NONMEM model pools these records into the ECOG = 0 reference, which is the convention the packaged model carries forward. A user simulating IPF-only cohorts can useECOG_GE1 = 0for all subjects without loss of fidelity vs the paper’s fit. -
NSCLC histology for IPF patients is encoded as
TUMTP_NSCLC_NONADENO = 0. Schmid 2017 Table 2 pools IPF subjects with “NSCLC of unknown histology” (415 / 1191 subjects = 34.8%) – IPF subjects have no tumour histology. The source model treats these as adenocarcinoma reference for the BIBF 1202 ka2 effect; the packaged model follows the same convention. -
units$dosing = "mg"vsunits$concentration = "nmol/L"is intentional and dimensionally mismatched. The paper reports doses in mg (mass) and plasma concentrations in nM (molar amount per volume) because the two analytes have closely-similar molecular weights and the molar scale preserves a clean parent/metabolite ratio. The model converts central mass to molar concentration explicitly inmodel()via the MW-derived conversion factorscf_nint = 1853(= 1000 ng/mL per mg/L * 1.853 nM per ng/mL, MW nintedanib 539.62 g/mol) andcf_bibf = 1903(MW BIBF 1202 525.59 g/mol). The convention-checkdosing_concentrationwarning is acknowledged and intentional; downstream simulations should keep doses in mg and read concentrations in nM. - Parameter values come from the SEQUENTIAL fit (Table 3 for nintedanib; Table S5 for BIBF 1202). Schmid 2017 also reports a simultaneous-fit alternative (Online Resource Table S7) where every parameter changes slightly (e.g., theta_CL = 875 vs 897, theta_V2 = 617 vs 465). The sequential fit was reported as the primary final model in the paper’s text and is what we package; the simultaneous fit is a consistency check and could be packaged separately as a sensitivity- analysis variant if a future use case requires it.
-
ffM(the fraction of nintedanib elimination that produces BIBF 1202 systemically, 0.000931, fixed) was carried over from an upstream healthy- volunteer IV nintedanib study (Schmid 2017 Online Resource Table S4, citing Dallinger et al. 2016 J Clin Pharmacol 56(11):1387-1394 [doi:10.1002/jcph.752]). The current paper used this value as a fixed input to the BIBF 1202 model and did not re-estimate it. Per the skill’s non-paper-provenance rule, the in-fileini()comment forlffmexplicitly cites Online Resource Table S4 as the source. -
V3/V2 = 0.0185is fixed from rat IV data (Schmid 2017 ref [14]). The paper notes “the ratio of V3/F-V2/F was fixed based on information observed in rats” without restating the rat-study citation in the main text; the rat data feed into the BIBF 1202 disposition volume. The fixed ratio is encoded vialvc_bibf <- fixed(log(8.6025))= log(465 * 0.0185). -
ALAG2 = ALAGis fixed. Schmid 2017 Online Resource Table S5 reportstheta_ALAG2ALAG = 1.00as fixed. Although the parameter is structurally identifiable, the authors fixed it to the parent ALAG without a substantial change in OFV (DeltaOFV = 1.282) “as besides the comparable estimates of ALAG2 and ALAG, the same absorption delay for both substances was considered plausible”.
Errata
- The on-disk PDF is named
Schmid_2018_Population_pharmacokinetics_of_nintedani_b579d1.pdfbut the paper itself has a 2017 acceptance date and CC-BY 2017 copyright (“Received: 20 June 2017 / Accepted: 10 October 2017 / Published online: 8 November 2017 The Author(s) 2017”). The packaged model file is namedSchmid_2017_nintedanib.Rper the skill convention (acceptance year) and per the operator’s sidecar-001 decision (response-001 option A, 2026-05-30). - The “Indian / Chinese / Taiwanese” ethnic-origin composite on
nintedanib F1 (Schmid 2017 Table 3) and the “Indian alone” composite on
BIBF 1202 F2 (Online Resource Table S5) are paper-specific groupings
with no obvious biological interpretation; they are empirical clustering
results from the covariate-search procedure. They are encoded faithfully
here so that any reanalysis can interrogate or refine the groupings –
see the canonical register entries
RACE_IND_CHI_TWN,RACE_KOREAN, andRACE_INDIANininst/references/covariate-columns.md.