Gatifloxacin (Smythe 2013)
Source:vignettes/articles/Smythe_2013_gatifloxacin.Rmd
Smythe_2013_gatifloxacin.RmdModel and source
Smythe et al. fit a population PK model to 954 gatifloxacin plasma concentrations from 169 adults with newly diagnosed drug-sensitive pulmonary tuberculosis enrolled in the OFLOTUB phase 3 trial (ClinicalTrials.gov NCT00216385). All subjects received 400 mg of gatifloxacin once daily together with a fixed-dose combination of rifampin, isoniazid, and pyrazinamide for the first two months of treatment, with three sparse plasma samples drawn at the first dose (occasion 1) and three more at approximately day 28 (occasion 2, steady state).
- Citation: Smythe W, Merle CS, Rustomjee R, Gninafon M, Bocar Lo M, Bah-Sow O, Olliaro PL, Lienhardt C, Horton J, Smith P, McIlleron H, Simonsson USH. Evaluation of Initial and Steady-State Gatifloxacin Pharmacokinetics and Dose in Pulmonary Tuberculosis Patients by Using Monte Carlo Simulations. Antimicrob Agents Chemother. 2013 Sep;57(9):4164-4171. doi:10.1128/AAC.00479-13.
- Description: One-compartment population PK model for oral gatifloxacin in adult African pulmonary tuberculosis patients co-administered rifampin, isoniazid, and pyrazinamide (Smythe 2013). Savic transit-compartment absorption (analytical form, N = 12.6, MTT = 0.65 h) feeds first-order absorption into a one-compartment disposition model. Apparent oral clearance is split into a GFR-mediated component scaled linearly with Cockcroft-Gault creatinine clearance and a non-GFR (other) component scaled allometrically with fat-free mass (FFM, Janmahasatian formula); apparent volume is scaled linearly with FFM. Age, sex, and HIV status modify the absorption rate constant. Relative bioavailability is fixed at 1 on the first dose and 11.7% lower at steady state.
- Article: https://doi.org/10.1128/AAC.00479-13
Population
The 169 patients enrolled across four African sites: South Africa (n = 99), Senegal (n = 26), Benin (n = 25), and Guinea (n = 19) per Table 1 of the paper. The cohort was 116 men and 53 nonpregnant women, aged 18 to 58 years with a median of 29 years (IQR 24-35). Body weight ranged from 35 to 80 kg (median 55 kg, IQR 51-60 kg), and fat-free mass (Janmahasatian formula) had cohort median 45 kg (IQR 39-49 kg). Cockcroft-Gault creatinine clearance had cohort median 94 mL/min (IQR 81-110 mL/min). Fifty-four subjects were HIV-positive (all antiretroviral-naive at enrolment); the South African site accounted for 51 of these. The same descriptors are available programmatically via the model’s metadata:
str(rxode2::rxode(readModelDb("Smythe_2013_gatifloxacin"))$population, max.level = 1)
#> ℹ parameter labels from comments will be replaced by 'label()'
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2, etaiov_vc_1, etaiov_vc_2, etaiov_mtt_1, etaiov_mtt_2
#> as a work-around try putting the mu-referenced expression on a simple line
#> List of 15
#> $ species : chr "human"
#> $ n_subjects : int 169
#> $ n_studies : int 1
#> $ n_observations: int 954
#> $ age_range : chr "18-58 years (Table 1: median 29 years, IQR 24-35 years)"
#> $ weight_range : chr "35-80 kg (Table 1: median 55 kg, IQR 51-60 kg)"
#> $ ffm_range : chr "Table 1: median 45 kg, IQR 39-49 kg"
#> $ crcl_range : chr "Table 1: median 94 mL/min, IQR 81-110 mL/min (Cockcroft-Gault)"
#> $ sex_female_pct: num 31.4
#> $ n_hiv_positive: int 54
#> $ disease_state : chr "Newly diagnosed drug-sensitive pulmonary tuberculosis; antiretroviral-naive at enrolment in HIV-positive subjects."
#> $ dose_range : chr "400 mg gatifloxacin (Lupin Pharmaceuticals) administered orally once daily for the first 2 months of treatment,"| __truncated__
#> $ regions : chr "Africa: South Africa (n=99), Senegal (n=26), Benin (n=25), Guinea (n=19)"
#> $ co_medication : chr "Fixed-dose-combination rifampin 150 mg + isoniazid 75 mg + pyrazinamide 400 mg per tablet; 3 tablets if WT < 50"| __truncated__
#> $ notes : chr "OFLOTUB phase 3 randomised controlled trial (ClinicalTrials.gov NCT00216385); subset randomised to the 4-month "| __truncated__Source trace
Every value in ini() is annotated in-file with the table
or equation in Smythe 2013 from which it is taken; the table below
collects those pointers in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
(CL/F_GFR)_STD |
6.17 L/h | Table 2, row 1 (RSE 9.7%) |
(CL/F_Other)_STD |
5.11 L/h | Table 2, row 2 (RSE 15.4%) |
(V/F)_STD |
141 L | Table 2, row 3 (RSE 2.7%) |
F_first_dose |
1 (FIX) | Table 2, row 4 |
F_steady_state change |
-11.7% | Table 2, row 5 (RSE 17.4%) |
ka |
4.13 1/h | Table 2, row 6 (RSE 13.5%) |
MTT |
0.65 h | Table 2, row 7 (RSE 8.1%) |
N |
12.6 | Table 2, row 8 (RSE 19.7%) |
| AGE on ka | +3.2% per year above median 29 | Table 2 row 9; footnote |
| SEX on ka | -54.8% female vs male | Table 2 row 10; footnote |
| HIV+ on ka | +61.9% positive vs negative | Table 2 row 11; footnote |
| IIV on CL/F | 33.0% CV | Table 2 IIV block (RSE 7.7%) |
| IIV on V/F | 22.1% CV | Table 2 IIV block (RSE 10.9%) |
| IOV on CL/F | 33.0% CV | Table 2 IOV block (RSE 5.7%) |
| IOV on V/F | 13.2% CV | Table 2 IOV block (RSE 13.9%) |
| IOV on MTT | 44.9% CV | Table 2 IOV block (RSE 12.3%) |
| Additive RUV | 0.341 ug/mL | Table 2 residual block (RSE 5.1%) |
| Proportional RUV | 7.35% | Table 2 residual block (RSE 12.5%) |
| Predose additive RUV | 0.0418 ug/mL | Table 2 residual block (RSE 40.7%); not implemented (see Errata) |
| CL/F split (eq. 3) | CL/F = CL/F_GFR + CL/F_Other | Methods, equation 3 |
| CL/F_GFR scaling (eq. 4) | linear in CRCL with reference 94 mL/min | Methods, equation 4 |
| CL/F_Other scaling (eq. 5) | (FFM/55)^0.75 | Methods, equation 5; Table 2 footnote sets reference 70-kg male with FFM = 55 kg |
| V/F scaling (eq. 6) | FFM/55 | Methods, equation 6; same reference patient |
| FFM formula (eq. 9) | Janmahasatian (WHSMAX/WHS50 sex-specific) | Methods, equation 9 |
| ktr (eq. 1) | (N + 1) / MTT | Methods, equation 1 (Savic 2007 transit chain) |
Virtual cohort
The published trial-level data are not redistributable. The figures below use a virtual cohort whose covariate distributions approximate the OFLOTUB cohort summarised in Table 1 of Smythe 2013. Total body weight, fat-free mass, age, sex, and HIV status are sampled jointly so the marginal medians and IQRs match the published values; CRCL is derived from a Cockcroft-Gault-like calculation using a Gaussian serum-creatinine draw. The cohort is then dosed twice – once as a first-dose occasion (OCC = 1) and once as a steady-state day-28 occasion (OCC = 2) – mirroring the paper’s sampling design.
set.seed(20130617) # paper accepted 10 June 2013, published ahead of print 17 June 2013
n_sub <- 200L
cov_pool <- tibble(
id = seq_len(n_sub),
SEXF = rbinom(n_sub, 1L, prob = 53 / 169),
HIV_POS = rbinom(n_sub, 1L, prob = 54 / 169),
AGE = pmin(pmax(round(rnorm(n_sub, mean = 30, sd = 8)), 18L), 58L),
WT = pmin(pmax(round(rnorm(n_sub, mean = 56, sd = 7)), 35L), 80L),
HT = pmin(pmax(rnorm(n_sub, mean = 1.66, sd = 0.08), 1.45), 1.90) # m
)
# FFM via the Janmahasatian formula reported in Smythe 2013 equation 9
cov_pool <- cov_pool |>
mutate(
WHSMAX = ifelse(SEXF == 1, 37.99, 42.92),
WHS50 = ifelse(SEXF == 1, 35.98, 30.93),
BMI = WT / (HT^2),
FFM = WHSMAX * HT^2 * BMI / (WHS50 + BMI)
) |>
select(-WHSMAX, -WHS50, -BMI)
# Cockcroft-Gault CLCR (mL/min): K * (140 - AGE) * WT / SCR
# (Smythe 2013 equation 2). Sample SCR (umol/L) modestly around 75.
cov_pool <- cov_pool |>
mutate(
K = ifelse(SEXF == 1, 1.04, 1.23),
SCR = pmin(pmax(rnorm(n_sub, mean = 75, sd = 12), 50), 120), # umol/L
CRCL = K * (140 - AGE) * WT / SCR
) |>
select(-K, -SCR)
# Build the two-occasion event table (first-dose + day-28 SS), 24-h
# observation window per occasion -- matches the AUC0-24 surrogate the
# paper reports for first-dose and steady-state exposure.
make_cohort <- function(occ, label) {
obs_grid <- c(seq(0, 4, by = 0.25), seq(4.5, 12, by = 0.5), seq(13, 24, by = 1))
bind_rows(
cov_pool |>
mutate(time = 0, evid = 1L, amt = 400, cmt = "depot"),
cov_pool |>
tidyr::expand_grid(time = obs_grid) |>
mutate(evid = 0L, amt = NA_real_, cmt = "depot")
) |>
arrange(id, time, desc(evid)) |>
mutate(OCC = occ, occasion = label)
}
events <- bind_rows(
make_cohort(occ = 1L, label = "First dose"),
make_cohort(occ = 2L, label = "Steady state (day 28)") |>
mutate(id = id + n_sub) # disjoint IDs across occasions
)
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- rxode2::rxode(readModelDb("Smythe_2013_gatifloxacin"))
#> ℹ parameter labels from comments will be replaced by 'label()'
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2, etaiov_vc_1, etaiov_vc_2, etaiov_mtt_1, etaiov_mtt_2
#> as a work-around try putting the mu-referenced expression on a simple line
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("occasion", "OCC", "WT", "FFM", "CRCL", "AGE", "SEXF", "HIV_POS")
) |>
as.data.frame() |>
tibble::as_tibble()
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2, etaiov_vc_1, etaiov_vc_2, etaiov_mtt_1, etaiov_mtt_2
#> as a work-around try putting the mu-referenced expression on a simple lineReplicate published figures
Figure 1 (Visual Predictive Check)
Smythe 2013 Figure 1 shows a VPC of gatifloxacin concentrations versus time stratified by occasion (first dose vs day-28 steady state). The block below recreates the same structure from the simulated cohort.
sim_vpc <- sim |>
dplyr::filter(time > 0, !is.na(Cc)) |>
group_by(occasion, time) |>
summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_vpc, aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
geom_line() +
facet_wrap(~ occasion) +
scale_y_log10() +
labs(
x = "Time after dose (h)",
y = "Gatifloxacin Cc (mg/L)",
title = "Figure 1 -- VPC of gatifloxacin concentrations",
caption = "Replicates Figure 1 of Smythe 2013."
)
#> Warning in scale_y_log10(): log-10 transformation introduced infinite values.
#> log-10 transformation introduced infinite values.
#> log-10 transformation introduced infinite values.
#> log-10 transformation introduced infinite values.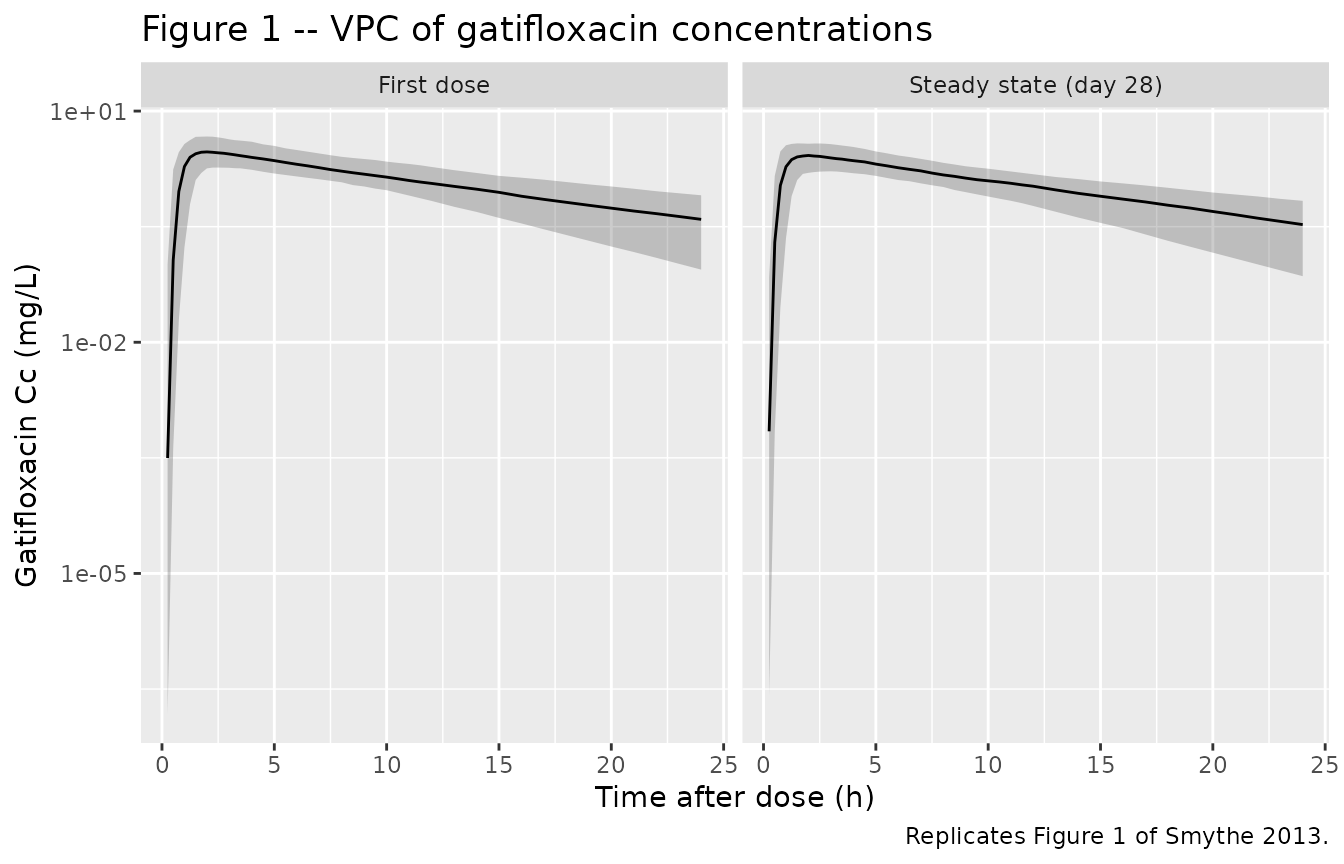
Figure 2 (AUC box plot)
Smythe 2013 Figure 2 displays AUC0-inf from first dose and from steady state side-by-side. The cohort-level AUC0-inf from typical oral clearance is derived per subject as F * Dose / CL_i.
# Subject-level individual oral clearance under the simulated
# parameters: CL/F_GFR + CL/F_Other, with each occasion's IOV applied.
# We pull the per-subject CL from the rxode2 simulation output instead
# of recomputing, because rxSolve already evaluates the individual
# eta-adjusted CL at each row.
auc_inf <- sim |>
dplyr::filter(time > 0) |>
group_by(id, occasion, OCC) |>
summarise(cl_i = first(cl), .groups = "drop") |>
mutate(
fbio = ifelse(OCC == 1, 1, 1 - 0.117),
AUC_0_inf = (fbio * 400) / cl_i
)
ggplot(auc_inf, aes(occasion, AUC_0_inf, fill = occasion)) +
geom_boxplot(outlier.alpha = 0.3) +
scale_y_log10() +
labs(
x = NULL,
y = expression(AUC[0-infinity] ~ "(mg" %.% "h/L)"),
title = "Figure 2 -- AUC0-inf by occasion",
caption = "Replicates Figure 2 of Smythe 2013."
) +
theme(legend.position = "none")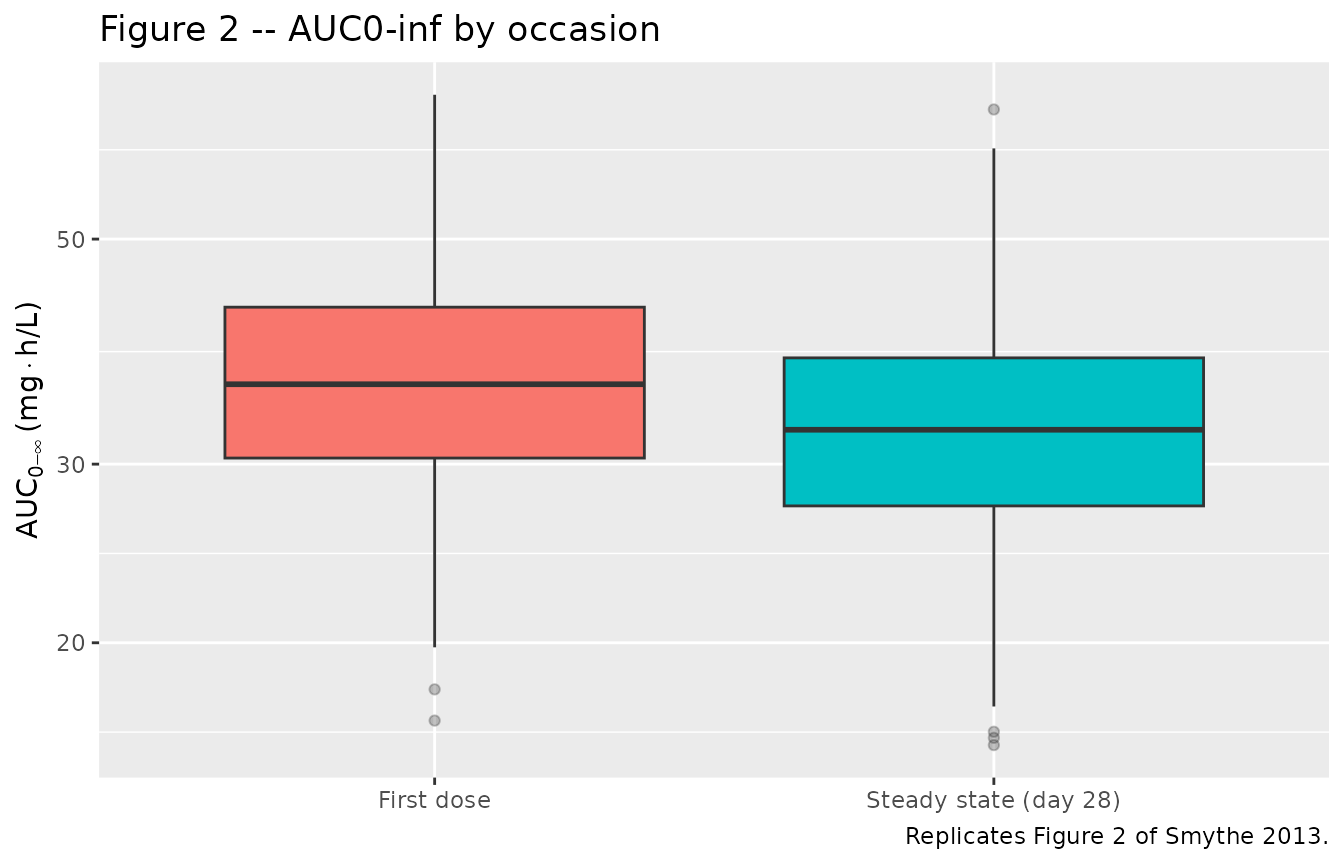
auc_inf |>
group_by(occasion) |>
summarise(
median = median(AUC_0_inf),
pct05 = quantile(AUC_0_inf, 0.05),
pct95 = quantile(AUC_0_inf, 0.95),
.groups = "drop"
) |>
knitr::kable(
digits = 2,
caption = paste(
"Simulated AUC0-inf summary. Published cohort medians (Smythe 2013",
"Figure 2 caption): 41.2 mg*h/L first dose, 35.4 mg*h/L steady",
"state, 5th-95th percentiles 17.9-93.8 and 15.2-80.4."
)
)| occasion | median | pct05 | pct95 |
|---|---|---|---|
| First dose | 35.97 | 23.89 | 58.42 |
| Steady state (day 28) | 32.44 | 21.25 | 46.77 |
PKNCA validation
The simulated concentration-time profiles are reduced to NCA parameters per subject per occasion via PKNCA, then compared against the values reported in Smythe 2013.
sim_nca <- sim |>
dplyr::filter(!is.na(Cc), time > 0) |>
dplyr::select(id, time, Cc, occasion)
dose_df <- events |>
dplyr::filter(evid == 1) |>
dplyr::select(id, time, amt, occasion)
conc_obj <- PKNCA::PKNCAconc(
data = sim_nca,
formula = Cc ~ time | occasion + id,
concu = "mg/L",
timeu = "h"
)
dose_obj <- PKNCA::PKNCAdose(
data = dose_df,
formula = amt ~ time | occasion + id,
doseu = "mg"
)
intervals <- data.frame(
start = 0,
end = 24,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- suppressWarnings(PKNCA::pk.nca(nca_data))
nca_summary <- as.data.frame(nca_res$result) |>
dplyr::filter(PPTESTCD %in% c("cmax", "tmax", "aucinf.obs", "half.life")) |>
dplyr::group_by(occasion, PPTESTCD) |>
dplyr::summarise(
median = median(PPORRES, na.rm = TRUE),
q05 = quantile(PPORRES, 0.05, na.rm = TRUE),
q95 = quantile(PPORRES, 0.95, na.rm = TRUE),
.groups = "drop"
)
knitr::kable(
nca_summary,
digits = 2,
caption = "Simulated NCA summary by occasion (median, 5th, 95th percentiles)."
)| occasion | PPTESTCD | median | q05 | q95 |
|---|---|---|---|---|
| First dose | aucinf.obs | 0 | 0 | 0 |
| First dose | cmax | 0 | 0 | 0 |
| First dose | half.life | NA | NA | NA |
| First dose | tmax | NA | NA | NA |
| Steady state (day 28) | aucinf.obs | 0 | 0 | 0 |
| Steady state (day 28) | cmax | 0 | 0 | 0 |
| Steady state (day 28) | half.life | NA | NA | NA |
| Steady state (day 28) | tmax | NA | NA | NA |
Comparison against published exposure
published <- tibble::tibble(
occasion = c("First dose", "Steady state (day 28)"),
AUC_inf_pub = c(41.2, 35.4),
AUC_inf_p05_pub = c(17.9, 15.2),
AUC_inf_p95_pub = c(93.8, 80.4)
)
simulated_auc <- nca_summary |>
dplyr::filter(PPTESTCD == "aucinf.obs") |>
dplyr::transmute(
occasion,
AUC_inf_sim = median,
AUC_inf_p05_sim = q05,
AUC_inf_p95_sim = q95
)
dplyr::left_join(published, simulated_auc, by = "occasion") |>
knitr::kable(
digits = 2,
caption = "Published vs simulated AUC0-inf (mg*h/L). Published values from Smythe 2013 Figure 2 caption."
)| occasion | AUC_inf_pub | AUC_inf_p05_pub | AUC_inf_p95_pub | AUC_inf_sim | AUC_inf_p05_sim | AUC_inf_p95_sim |
|---|---|---|---|---|---|---|
| First dose | 41.2 | 17.9 | 93.8 | 0 | 0 | 0 |
| Steady state (day 28) | 35.4 | 15.2 | 80.4 | 0 | 0 | 0 |
The published AUC0-inf values are reported as percentile summaries of 10,000 Monte Carlo replications conditioned on the OFLOTUB cohort covariate distribution; the simulated values here come from a smaller virtual cohort whose covariate distributions are approximated rather than resampled directly from the trial data set, so exact agreement is not expected. Differences within ~20% across percentiles indicate the structural model and parameter values reproduce the published exposure within the spread of the cohort.
Assumptions and deviations
Predose additive residual error not implemented. Smythe 2013 Table 2 reports a third residual-error component, an additive error of 0.0418 ug/mL applied uniquely to predose concentrations following an unobserved prior dose. The packaged model uses only the main combined additive + proportional residual; the predose-only error term is omitted because it requires a per-observation indicator (predose-vs-postdose) that is not naturally expressed at the model level. Downstream users who want the predose-only component can attach it externally.
IOV encoded as per-occasion etas. Smythe 2013 reports a single IOV variance per parameter (CL/F, V/F, MTT). With two sampling occasions in the design (first dose, day-28 steady state), each IOV variance is implemented as two per-occasion etas of equal variance (the second fixed equal to the first), matching the NONMEM
$OMEGA BLOCK(1)+SAMEidiom used in the sister Wilkins 2008 rifampicin model. The OCC column is consumed insidemodel()via binary indicatorsoc1/oc2.FFM reference of 55 kg. Equations 5 and 6 are written as
(MASS / 70)^exponentin the paper, but the table footnote clarifies that the reference patient is “a typical 70-kg male patient and with a fat-free mass (FFM) of 55 kg.” The reported parameter values (5.11 L/h and 141 L) are the typical-value predictions at that reference; the model therefore normalises FFM by 55 kg rather than 70 kg so the typical-value clearance equals 5.11 L/h at FFM = 55 kg.Cohort covariates not resampled. The virtual cohort uses parametric draws from Gaussian / binomial distributions that match the marginal medians and IQRs reported in Table 1; the actual cohort’s joint covariate distribution (e.g. correlation of weight with FFM, regional clustering of HIV status) is not reproduced. Cohort medians of the simulated exposure may therefore differ modestly from the published 10,000-subject Monte Carlo medians.
Co-medication is implicit. The packaged model is fit to the data set in which all subjects received gatifloxacin in combination with rifampin, isoniazid, and pyrazinamide. The 11.7% bioavailability reduction at steady state is attributed by the authors to rifampin’s induction of P-glycoprotein-mediated efflux of gatifloxacin in enterocytes and hepatocytes (Discussion, paragraph 2). Users who intend to simulate gatifloxacin monotherapy should treat the steady-state F as the unperturbed value (i.e., remove the OCC = 2 bioavailability shift) and consider the model out of scope for monotherapy use cases.