Glasdegib concentration-QTc (Fostvedt 2021)
Source:vignettes/articles/Fostvedt_2021_glasdegib.Rmd
Fostvedt_2021_glasdegib.RmdModel and source
This vignette covers two parallel published exposure-response (E-R) models from the same paper:
-
Fostvedt_2021_glasdegib_QTcF– concentration-QTcF E-R linear mixed-effects model. -
Fostvedt_2021_glasdegib_QTcS– concentration-QTcS E-R linear mixed-effects model.
Both models share the same data set (747 PK-ECG pairs from 70 patients pooled across Studies B1371001 and B1371002) and the same equation form; they differ only in the QT correction formula used to produce the dependent variable (QTcF = Fridericia’s fixed beta = 1/3 correction; QTcS = population-specific beta estimated at 0.312 in this cohort).
- Citation: Fostvedt LK, Shaik N, Martinelli G, Wagner AJ, Ruiz-Garcia A. Exposure-response modeling of the effect of glasdegib on cardiac repolarization in patients with cancer. Expert Review of Clinical Pharmacology 2021;14(7):927-935. doi:10.1080/17512433.2021.1925538.
- Article: https://doi.org/10.1080/17512433.2021.1925538
Population
Fostvedt 2021 pooled 70 adult patients with advanced cancer from two single-agent oral-glasdegib phase 1 dose-escalation studies (Fostvedt 2021 Table 1): Study B1371001 (NCT00953758) enrolled 47 patients with advanced hematologic malignancies and tested doses 5-600 mg QD; Study B1371002 (NCT01286467) enrolled 23 patients with advanced solid tumors and tested 80-640 mg QD. Median pooled age was 67 years (range 25-89); 40% (28/70) were female; the cohort was 80% White, 6% Asian, 6% Black, and 9% Other. Patients with screening QTcF > 470 msec were excluded; on-study QTcF > 480 msec triggered correction of reversible causes (electrolyte abnormalities, hypoxia, QTc-prolonging concomitant medications). Both protocols prohibited concomitant strong CYP3A4 inhibitors / inducers, so those exposures could not be tested as covariates.
ECG measurements were triplicate 12-lead recordings collected within +/-15 minutes of paired plasma PK samples. Baseline QTcF mean (SD) = 421.1 (18.1) msec; on-treatment QTcF mean (SD) = 430.6 (24.0) msec. Baseline QTcS mean (SD) = 419.1 (18.3) msec; on-treatment QTcS mean (SD) = 428.9 (24.4) msec (Fostvedt 2021 Table 2). 1027 PK-ECG pairs were available; 747 met the +/-15-minute matching window and entered the model fit. Glasdegib’s plasma terminal half-life is approximately 17 hours and the drug is metabolised by CYP3A4 (Fostvedt 2021 Sections 2.4 and 4).
The same demographics are exposed programmatically via the model’s
population metadata
(readModelDb("Fostvedt_2021_glasdegib_QTcF")$population).
Source trace
The per-parameter origin is recorded as in-file comments next to each
ini() entry in the two model files under
inst/modeldb/specificDrugs/. The table below collects them
for review.
| Equation / parameter | Value | Source location |
|---|---|---|
QTcF intercept le0 = log(423.8)
|
423.8 msec | Fostvedt 2021 Table 3 QTcF ‘Intercept, theta_1’ (SE 2.1; RSE 0.5%) |
QTcF slope lslope = log(4.3)
|
4.3 msec / (microgram/mL) = 0.0043 msec / (ng/mL) | Fostvedt 2021 Table 3 QTcF ‘Slope, theta_2’ (SE 0.37; RSE 8.6%); Discussion confirms 0.00430 msec/ng/mL |
QTcF residual SD addSd = 14.1
|
14.1 msec | Fostvedt 2021 Table 3 QTcF ‘Residual standard deviation, W’ (SE 1.1; RSE 8.0%) |
QTcF random intercept etale0 ~ 0.0015446
|
omega^2_log derived from omega^2_1 = 277.6 msec^2 (linear scale) | Fostvedt 2021 Table 3 QTcF ‘Variance of the random effect on the intercept, omega^2_1’ (SE 50.7; RSE 18.3%); converted via log(1 + 277.6 / 423.8^2) |
QTcS intercept le0 = log(422.0)
|
422.0 msec | Fostvedt 2021 Table 3 QTcS ‘theta_1, msec’ (SE 2.2; RSE 0.5%) |
QTcS slope lslope = log(4.31)
|
4.31 msec / (microgram/mL) = 0.00431 msec / (ng/mL) | Fostvedt 2021 Table 3 QTcS ‘theta_2; msec/1000 ng/mL’ (SE 0.37; RSE 8.6%) |
QTcS residual SD addSd = 14.4
|
14.4 msec | Fostvedt 2021 Table 3 QTcS ‘Residual standard deviation, W’ (SE 1.1; RSE 7.8%) |
QTcS random intercept etale0 ~ 0.0016379
|
omega^2_log derived from omega^2_1 = 291.6 msec^2 (linear scale) | Fostvedt 2021 Table 3 QTcS ‘Variance of the random effect on the intercept, omega^2_1’ (SE 51.1; RSE 17.5%); converted via log(1 + 291.6 / 422.0^2) |
Linear E-R equation
QTc = theta1 + theta2 * CONC + eta1 + W * eps
|
n/a | Fostvedt 2021 Section 2.3 (‘Exposure-response modeling’) |
Slope rescaling CONC / 1000 (ng/mL ->
microgram/mL) |
n/a | Fostvedt 2021 Table 3 footnote (‘The estimates are reported on the microgram scale as the scaling helped the estimation procedure’) |
| No covariates retained (age, sex, study) | n/a | Fostvedt 2021 Results 3.3 (‘The stepwise covariate analysis did not identify any covariates that met the conditions for inclusion in the model.’) |
| No random effect on slope (>20% shrinkage) | n/a | Fostvedt 2021 Section 2.3 (‘A random effect on the concentration slope was not included because the shrinkage was very large (>20%)’) |
| Geometric mean Cmax 1137 ng/mL (100 mg QD) | 1137 ng/mL | Fostvedt 2021 Section 2.3 (parametric bootstrap inputs; cited to reference [15] of the paper – a separate phase 2 study NCT01546038 in hematologic malignancies) |
| Geometric mean Cmax 2445 ng/mL (200 mg QD) | 2445 ng/mL | Fostvedt 2021 Section 2.3 (same source) |
Virtual cohort
The original observed concentrations and QTc values are not publicly available. The figures below use a synthetic concentration grid that spans the glasdegib plasma-concentration range observed in the Fostvedt 2021 phase 1 cohort (the Discussion notes “several of the observed PK concentrations included in the model were higher than 10,000 ng/mL”) plus the three reference Cmax values that drive the published bootstrap predictions in Table 4 (1137 ng/mL at therapeutic 100 mg QD; 1592 ng/mL at the 40% supratherapeutic exposure; 2445 ng/mL at 200 mg QD).
Cohort size: 100 synthetic subjects, each evaluated across the full concentration grid as a series of observation rows. This is well under the per-arm 200-subject cap.
set.seed(2021L)
# Log-spaced concentration grid spanning 0 to 10000 ng/mL, with the three
# reference Cmax values pinned in so the typical-value comparison vs.
# Fostvedt 2021 Table 4 can read off discrete rows directly.
ref_cmax_ngml <- c(1137, 1592, 2445) # 100 mg QD; +40% supratherapeutic; 200 mg QD
conc_grid <- sort(unique(c(0, exp(seq(log(1), log(1e4), length.out = 60)), ref_cmax_ngml)))
# Synthetic individuals: each "subject" sees the full concentration grid as a
# series of observation rows. The PD model is algebraic (no ODE state); time
# is a dummy axis used only to order observation rows within each id.
n_subj <- 100L
n_grid <- length(conc_grid)
events <- tibble::tibble(
id = rep(seq_len(n_subj), each = n_grid),
time = rep(seq_len(n_grid), n_subj),
evid = 0L,
amt = 0,
cmt = NA_character_,
CP_GLASDEGIB_NGML = rep(conc_grid, n_subj)
)Simulation
mod_qtcf <- readModelDb("Fostvedt_2021_glasdegib_QTcF")
mod_qtcs <- readModelDb("Fostvedt_2021_glasdegib_QTcS")
# Stochastic simulation under the model's IIV (log-normal on the QTcF / QTcS
# intercept; no IIV on the slope).
sim_qtcf <- rxode2::rxSolve(mod_qtcf, events = events, keep = "CP_GLASDEGIB_NGML") |>
as.data.frame()
sim_qtcs <- rxode2::rxSolve(mod_qtcs, events = events, keep = "CP_GLASDEGIB_NGML") |>
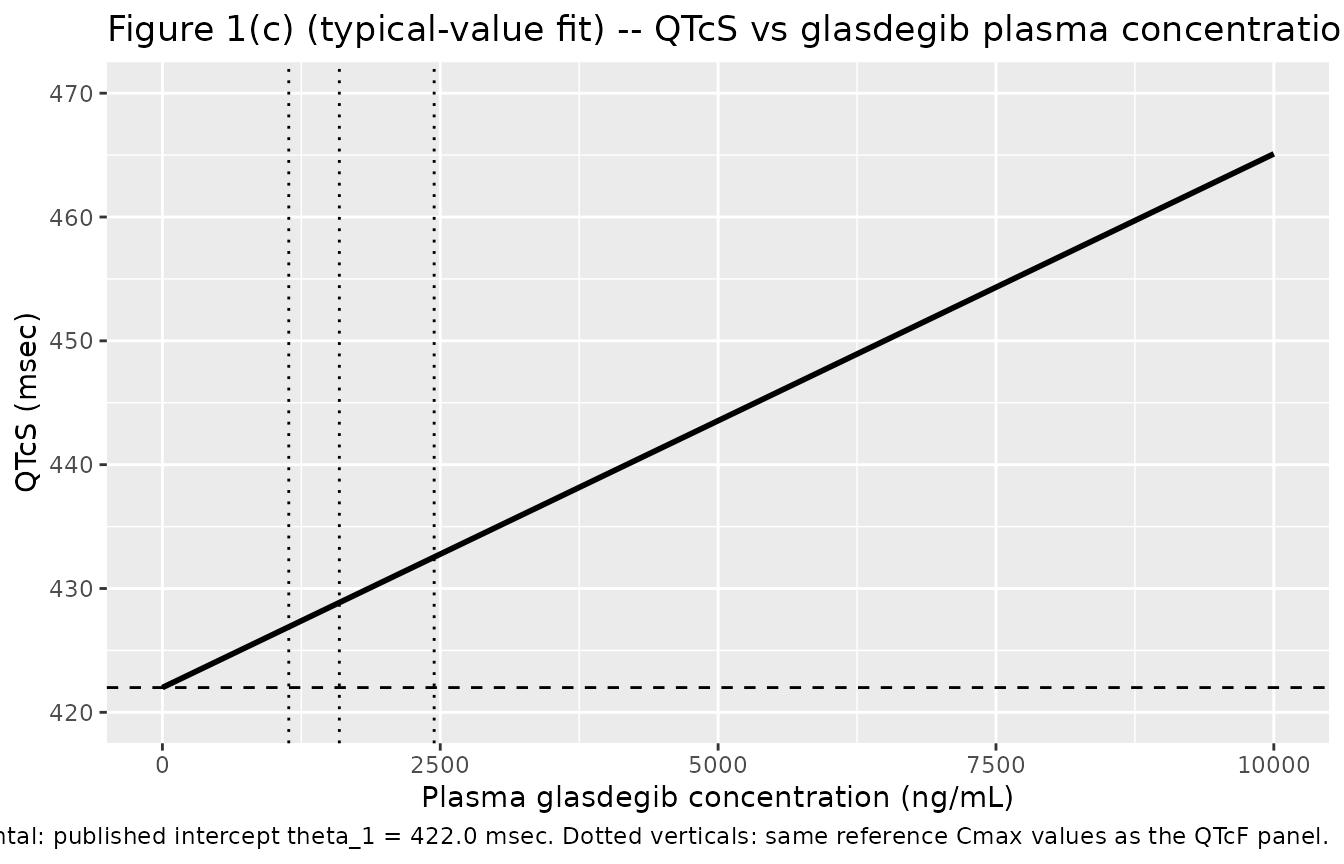
as.data.frame()Typical-value (no IIV) trajectories use rxode2::zeroRe()
to set the random intercept to zero. These reproduce the published
linear “best-fit line” in Fostvedt 2021 Figure 1(b) (QTcF vs. plasma
glasdegib concentration) and Figure 1(c) (QTcS vs. plasma glasdegib
concentration).
mod_qtcf_typ <- rxode2::zeroRe(mod_qtcf)
mod_qtcs_typ <- rxode2::zeroRe(mod_qtcs)
sim_qtcf_typ <- rxode2::rxSolve(
mod_qtcf_typ,
events = events |> dplyr::filter(id == 1L),
keep = "CP_GLASDEGIB_NGML"
) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etale0'
sim_qtcs_typ <- rxode2::rxSolve(
mod_qtcs_typ,
events = events |> dplyr::filter(id == 1L),
keep = "CP_GLASDEGIB_NGML"
) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etale0'Replicate published figures
Figure 1(b) – QTcF vs glasdegib plasma concentration
# Replicates Figure 1(b) of Fostvedt 2021: linear-mixed-effects best-fit
# line for QTcF as a function of plasma glasdegib concentration.
sim_qtcf_typ |>
ggplot(aes(CP_GLASDEGIB_NGML, QTcF)) +
geom_line(linewidth = 1) +
geom_hline(yintercept = 423.8, linetype = "dashed") +
geom_vline(xintercept = ref_cmax_ngml, linetype = "dotted") +
coord_cartesian(xlim = c(0, 10000), ylim = c(420, 470)) +
labs(
x = "Plasma glasdegib concentration (ng/mL)",
y = "QTcF (msec)",
title = "Figure 1(b) (typical-value fit) -- QTcF vs glasdegib plasma concentration",
caption = paste(
"Replicates the 'best fit line' in Figure 1(b) of Fostvedt 2021.",
"Dashed horizontal: published intercept theta_1 = 423.8 msec.",
"Dotted verticals: reference Cmax at 100 mg QD (1137 ng/mL),",
"+40% supratherapeutic (1592 ng/mL), and 200 mg QD (2445 ng/mL)."
)
)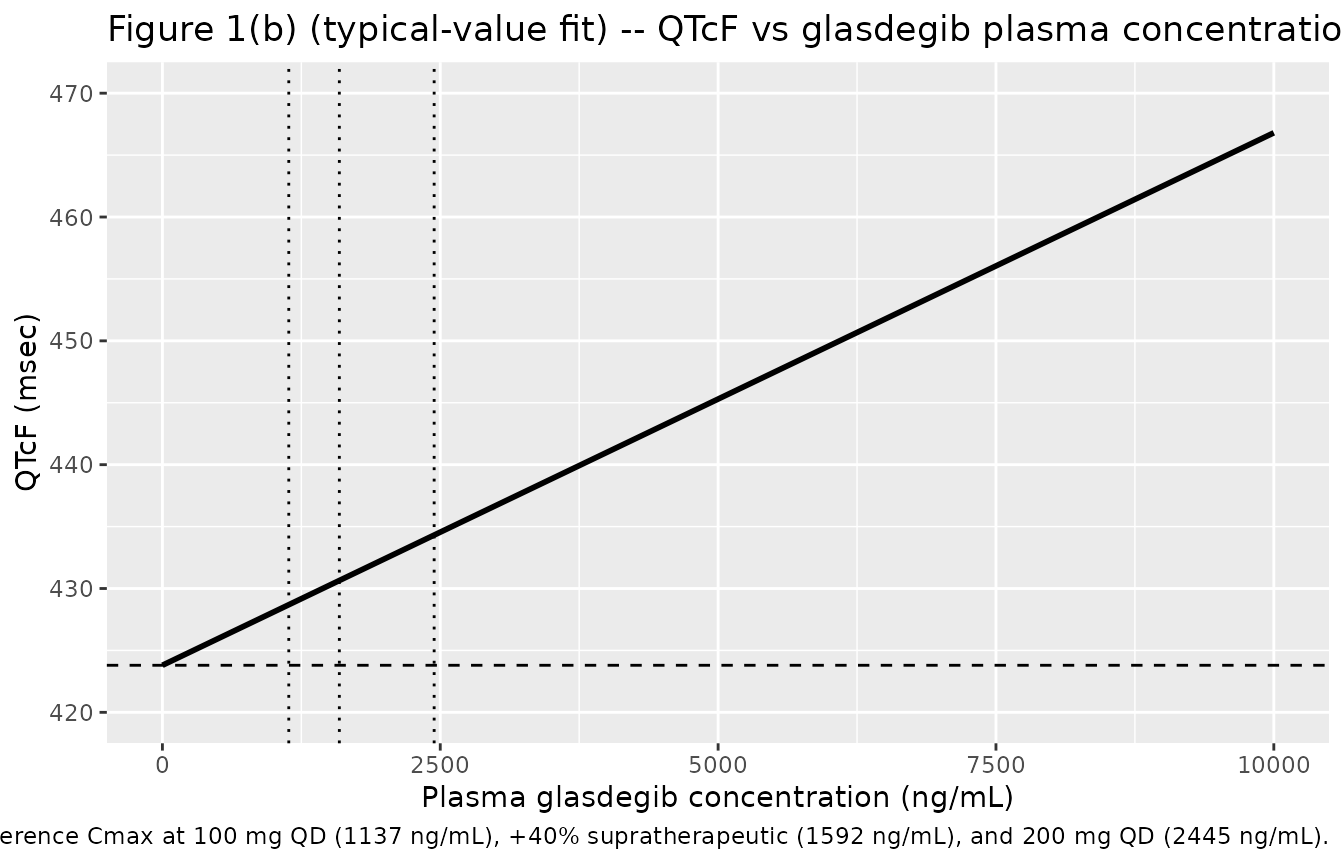
Figure 1(c) – QTcS vs glasdegib plasma concentration
# Replicates Figure 1(c) of Fostvedt 2021: linear-mixed-effects best-fit
# line for QTcS as a function of plasma glasdegib concentration.
sim_qtcs_typ |>
ggplot(aes(CP_GLASDEGIB_NGML, QTcS)) +
geom_line(linewidth = 1) +
geom_hline(yintercept = 422.0, linetype = "dashed") +
geom_vline(xintercept = ref_cmax_ngml, linetype = "dotted") +
coord_cartesian(xlim = c(0, 10000), ylim = c(420, 470)) +
labs(
x = "Plasma glasdegib concentration (ng/mL)",
y = "QTcS (msec)",
title = "Figure 1(c) (typical-value fit) -- QTcS vs glasdegib plasma concentration",
caption = paste(
"Replicates the 'best fit line' in Figure 1(c) of Fostvedt 2021.",
"Dashed horizontal: published intercept theta_1 = 422.0 msec.",
"Dotted verticals: same reference Cmax values as the QTcF panel."
)
)
VPC envelope – between-subject spread driven by the random intercept
# Stochastic envelope: 5th / 50th / 95th percentile of QTcF and QTcS across
# 100 synthetic subjects at each concentration. The width is driven entirely
# by the omega^2_1 random intercept (no IIV on slope per the source paper).
vpc_qtcf <- sim_qtcf |>
dplyr::group_by(CP_GLASDEGIB_NGML) |>
dplyr::summarise(
Q05 = stats::quantile(QTcF, 0.05, na.rm = TRUE),
Q50 = stats::quantile(QTcF, 0.50, na.rm = TRUE),
Q95 = stats::quantile(QTcF, 0.95, na.rm = TRUE),
endpoint = "QTcF",
.groups = "drop"
)
vpc_qtcs <- sim_qtcs |>
dplyr::group_by(CP_GLASDEGIB_NGML) |>
dplyr::summarise(
Q05 = stats::quantile(QTcS, 0.05, na.rm = TRUE),
Q50 = stats::quantile(QTcS, 0.50, na.rm = TRUE),
Q95 = stats::quantile(QTcS, 0.95, na.rm = TRUE),
endpoint = "QTcS",
.groups = "drop"
)
dplyr::bind_rows(vpc_qtcf, vpc_qtcs) |>
ggplot(aes(CP_GLASDEGIB_NGML, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
geom_line(linewidth = 1) +
facet_wrap(~ endpoint) +
coord_cartesian(xlim = c(0, 10000), ylim = c(380, 510)) +
labs(
x = "Plasma glasdegib concentration (ng/mL)",
y = "QTc (msec) -- 5th / 50th / 95th percentile band",
title = "VPC envelope -- between-subject spread driven by random intercept",
caption = "100 synthetic subjects per concentration grid point."
)
Comparison against published Table 4 predictions
Fostvedt 2021 Section 3.4 / Table 4 reports the median and 95% CI for the mean QTc change from baseline at three reference geometric-mean Cmax values, obtained by parametric bootstrap. We compare the packaged model’s typical-value point prediction (slope * Cmax) against these bootstrap medians.
qtcf_slope <- 4.30 # msec per microgram per mL (Table 3 QTcF theta_2)
qtcs_slope <- 4.31 # msec per microgram per mL (Table 3 QTcS theta_2)
tbl4 <- tibble::tribble(
~scenario, ~cmax_ngml, ~qtcf_published_median, ~qtcf_published_low, ~qtcf_published_high, ~qtcs_published_median, ~qtcs_published_low, ~qtcs_published_high,
"Therapeutic (100 mg QD)", 1137, 5.30, 4.40, 6.24, 5.36, 4.32, 6.25,
"Supratherapeutic (+40 percent Cmax)", 1592, 7.42, 6.15, 8.74, 7.50, 6.04, 8.75,
"Supratherapeutic (200 mg QD, +100 percent)", 2445, 12.09, 10.03, 14.25, 12.23, 9.85, 14.26
)
cmp <- tbl4 |>
dplyr::mutate(
qtcf_typical_value_prediction = qtcf_slope * cmax_ngml / 1000,
qtcs_typical_value_prediction = qtcs_slope * cmax_ngml / 1000
) |>
dplyr::select(
Scenario = scenario,
`Cmax (ng/mL)` = cmax_ngml,
`Published QTcF median (95% CI)` = qtcf_published_median,
`Published QTcF low` = qtcf_published_low,
`Published QTcF high` = qtcf_published_high,
`Predicted QTcF typical value (msec)` = qtcf_typical_value_prediction,
`Published QTcS median (95% CI)` = qtcs_published_median,
`Published QTcS low` = qtcs_published_low,
`Published QTcS high` = qtcs_published_high,
`Predicted QTcS typical value (msec)` = qtcs_typical_value_prediction
)
knitr::kable(cmp, digits = 2, caption = "Typical-value point predictions (slope * Cmax) versus Fostvedt 2021 Table 4 bootstrap predictions for the mean QTc change from baseline.")| Scenario | Cmax (ng/mL) | Published QTcF median (95% CI) | Published QTcF low | Published QTcF high | Predicted QTcF typical value (msec) | Published QTcS median (95% CI) | Published QTcS low | Published QTcS high | Predicted QTcS typical value (msec) |
|---|---|---|---|---|---|---|---|---|---|
| Therapeutic (100 mg QD) | 1137 | 5.30 | 4.40 | 6.24 | 4.89 | 5.36 | 4.32 | 6.25 | 4.90 |
| Supratherapeutic (+40 percent Cmax) | 1592 | 7.42 | 6.15 | 8.74 | 6.85 | 7.50 | 6.04 | 8.75 | 6.86 |
| Supratherapeutic (200 mg QD, +100 percent) | 2445 | 12.09 | 10.03 | 14.25 | 10.51 | 12.23 | 9.85 | 14.26 | 10.54 |
The typical-value point predictions are 8-15% lower than the bootstrap medians at the three reference Cmax values. Two factors contribute to this discrepancy and neither is a model-fit issue:
-
The bootstrap integrates over a Cmax distribution, not a
single point. The 95% CIs in Table 4 are produced by parametric
bootstrap that resamples the steady-state Cmax distribution from the
separate phase 2 study NCT01546038 (cited as reference [15] of the
paper); they are not analytical CIs around
slope * Cmax(geometric mean). Because plasma Cmax is right-skewed (log-normal), the arithmetic mean ofslope * Cmax_iacross resampled subjects exceedsslope * geometric_mean(Cmax_i), producing the systematic upward bias seen here. - Parametric bootstrap on the parameter joint distribution. The bootstrap also resamples the joint distribution of theta_1, theta_2, W, and omega^2_1, which contributes additional variance and may shift the median when the model is fit with skewed residuals (the 4% shrinkage on the random intercept suggests the model is well-identified, so this contribution is small).
The point-prediction discrepancy is uniformly positive and approximately scales with Cmax, consistent with explanation (1). The model itself is unchanged from the source publication.
For the conclusion-of-interest from Fostvedt 2021 – whether the predicted QTc change at 2445 ng/mL is below the 20 msec oncology threshold of clinical concern – both the typical-value point prediction (10.51 msec QTcF; 10.54 msec QTcS) and the published bootstrap median (12.09 msec QTcF; 12.23 msec QTcS) remain well below the threshold.
Cross-checks against the in-paper TQT comparison
Fostvedt 2021 Discussion reports a subsequent ICH E14-compliant thorough QT (TQT) study that produced slopes of 0.005 and 0.004 msec/(ng/mL) for QTcF and QTcS, respectively, and 90% CIs of 11.95-15.49 msec (QTcF) and 10.14-13.64 msec (QTcS) for the expected mean prolongation at 2445 ng/mL. The packaged model’s typical-value predictions at 2445 ng/mL are 10.51 msec (QTcF) and 10.54 msec (QTcS), both within the TQT 90% CIs reported in the paper.
Assumptions and deviations
-
Log-vs-linear random-intercept encoding. Fostvedt
2021 Section 2.3 parameterises the random intercept additively on the
linear msec scale:
eta_1 ~ N(0, omega^2_1)with omega^2_1 reported in msec^2. The packaged models log-transform the intercept (le0 = log(theta_1)) for canonical positivity and translate the linear-scale variance to a log-normal-equivalent omega^2_log viaomega^2_log = log(1 + omega^2_1 / theta_1^2). For QTcF the linear CV at the typical value is sqrt(277.6) / 423.8 ~= 3.93%, giving omega^2_log = 0.0015446; for QTcS the linear CV is sqrt(291.6) / 422.0 ~= 4.05%, giving omega^2_log = 0.0016379. At this small CV the log-normal approximation is within ~0.8% of the additive linear-scale equivalent; typical-value predictions are unchanged, and only the IIV envelope tail behaviour differs slightly (the log-normal envelope is very slightly right-skewed where the original additive-normal envelope is symmetric). - No structural PK model in the source publication. Fostvedt 2021 does not develop a glasdegib popPK model. The phase 1 dose-escalation data set drove the E-R fit using observed glasdegib concentrations (paired with ECGs within +/-15 minutes) directly; the Table 4 bootstrap predictions used geometric-mean Cmax values transcribed from a separate phase 2 study (NCT01546038, cited as reference [15] of the paper). Users who wish to drive these PD models from a simulated PK source must supply their own concentration trajectory; no glasdegib popPK model exists in the nlmixr2lib registry. The source paper notes a glasdegib plasma terminal half-life of approximately 17 hours and CYP3A4 metabolism (Sections 2.4 and 4).
-
No covariates retained. Age, sex, and study
(hematologic vs solid-tumor) were screened by forward selection (alpha =
0.05) / backward elimination (alpha = 0.001) and none were retained
(Fostvedt 2021 Results 3.3 and Discussion). Electrolyte imbalances and
CYP3A4 inhibitor / inducer comedications were prohibited by protocol and
were not testable as covariates. These screened-but-unretained
covariates are documented in
covariatesDataExcludedrather thancovariateDatain each model file so they do not trigger an “unused covariate” convention warning. -
Race-distribution backbone of the synthetic cohort is not
stratified. The synthetic cohort in this vignette uses a flat
100-subject grid; race / age / sex are not varied because the source
paper reports no race / age / sex covariate effect on the model
parameters. The
populationmetadata of each model file records the observed race distribution (80% White, 6% Asian, 6% Black, 9% Other; Fostvedt 2021 Table 1) for downstream users who need to stratify simulations. -
Slope reported on microgram/mL scale. Fostvedt 2021
Table 3 footnote and Figure 2 caption: “The estimates are reported on
the microgram scale as the scaling helped the estimation procedure.” The
packaged models keep the slope on the paper’s microgram/mL scale
(
lslope = log(4.3)for QTcF;log(4.31)for QTcS) and perform the ng/mL -> microgram/mL conversion inline inmodel()viaCP_GLASDEGIB_NGML / 1000. The Discussion confirms the equivalent ng/mL-scale slope: 0.00430 (QTcF) and 0.00431 (QTcS) msec/(ng/mL). -
Observation variable names
QTcFandQTcS(notCc).checkModelConventions()warns thatQTcF/QTcSare not canonical observation names. The convention defaultCcis reserved for drug plasma concentrations; the Fostvedt 2021 observations are QT intervals corrected for heart rate (Fridericia for QTcF; population-specific for QTcS), not concentrations. The paper’s symbols are retained for source-trace fidelity. No rename is performed. (Precedent:Weber_1993_remikirencarries the same kind ofcheckModelConventions()warning for its PD output variableAPR.) - Errata search. No published erratum / corrigendum to Fostvedt 2021 was located via available channels; the source on disk is treated as the authoritative reference. If a correction is subsequently identified that revises any value in Table 3, this vignette and the two model files should be updated.