Model and source
- Citation: Zhao W, Cella M, Della Pasqua O, Burger D, Jacqz-Aigrain E, on behalf of Pediatric European Network for Treatment of AIDS (PENTA) 15 study group. Population pharmacokinetics and maximum a posteriori probability Bayesian estimator of abacavir: application of individualized therapy in HIV-infected infants and toddlers. Br J Clin Pharmacol. 2012;73(4):641-648. doi:10.1111/j.1365-2125.2011.04121.x
- Description: Two-compartment population PK model for oral abacavir in HIV-infected infants and toddlers (Zhao 2012) developed on the PENTA 15 crossover trial of 8 mg/kg twice-daily vs 16 mg/kg once-daily dosing; CL/F scales with body weight via an estimated power exponent (1.14) referenced to the population median weight of 12 kg, and inter-occasion variability on CL/F is multiplexed by the binary OCC indicator across the BID (occasion 1) and QD (occasion 2) study phases.
- Article: https://doi.org/10.1111/j.1365-2125.2011.04121.x
Population
Zhao 2012 reports a population PK analysis of oral abacavir in 23 HIV type-1 infected infants and toddlers (12 male, 11 female; age 0.43-2.89 years, mean 1.8 years; weight 7.4-15.9 kg, mean 11.6 kg, median 12 kg) enrolled in the open-label PENTA 15 crossover study. Each child received abacavir 8 mg/kg twice daily (weeks 0-4) and then crossed over to abacavir 16 mg/kg once daily (weeks 4-8), with intensive plasma PK sampling at steady state in each phase. The cohort spanned France, Germany, Italy, Spain, and the United Kingdom. 347 plasma concentrations were available for modelling; 13.5% were below the lower limit of quantification (LLQ 0.015 mg/L) and were imputed at LLQ/2. The covariate screen tested age, sex, weight, height, body mass index, serum creatinine, and dose frequency; only weight on CL/F was retained in the final model (paper Tables 1-3).
The same information is available programmatically:
readModelDb("Zhao_2012_abacavir")$population after the
model is loaded.
Source trace
Per-parameter origin (also recorded as in-file comments next to each
ini() entry of
inst/modeldb/specificDrugs/Zhao_2012_abacavir.R):
| Equation / parameter | Value | Source location |
|---|---|---|
lka |
log(0.758) | Zhao 2012 Table 3 (Ka = 0.758 1/h) |
lcl |
log(13.4) | Zhao 2012 Table 3 (theta_4 = 13.4 L/h at 12 kg) |
lvc |
log(4.94) | Zhao 2012 Table 3 (V1/F = 4.94 L) |
lvp |
log(8.12) | Zhao 2012 Table 3 (V2/F = 8.12 L) |
lq |
log(1.25) | Zhao 2012 Table 3 (Q/F = 1.25 L/h) |
e_wt_cl |
1.14 | Zhao 2012 Table 3 (theta_5 = 1.14; estimated PWR exponent on WT for CL/F) |
| Reference WT (12 kg) | n/a | Zhao 2012 Results (cohort median used as the WT reference for the power model) |
etalcl |
0.03884 | Zhao 2012 Table 3 (IIV CL/F = 19.9% CV; omega^2 = log(1 + 0.199^2)) |
etalvp |
0.14977 | Zhao 2012 Table 3 (IIV V2/F = 40.2% CV; omega^2 = log(1 + 0.402^2)) |
etalq |
0.09120 | Zhao 2012 Table 3 (IIV Q/F = 30.9% CV; omega^2 = log(1 + 0.309^2)) |
etaiov_cl_1 |
0.04559 | Zhao 2012 Table 3 (IOV CL/F = 21.6% CV; omega^2 = log(1 + 0.216^2)); occasion-1 estimate |
etaiov_cl_2 |
fix(0.04559) | Zhao 2012 Table 3 (IOV CL/F shared variance across occasions; NONMEM
$OMEGA BLOCK(1) SAME translation) |
propSd |
0.141 | Zhao 2012 Table 3 (residual proportional = 14.1%) |
d/dt(depot), d/dt(central),
d/dt(peripheral1)
|
n/a | Zhao 2012 Methods (two-compartment with first-order oral absorption and first-order elimination) |
Cc <- central / vc |
n/a | Standard linear-CL parameterisation; dose mg, volume L -> mg/L = ug/mL |
Cc ~ prop(propSd) |
n/a | Zhao 2012 Results (“Residual variability was best described by a proportional model”) |
Virtual cohort
The virtual cohort below reproduces the PENTA 15 crossover at the
cohort-median weight of 12 kg: each of 60 simulated subjects receives
five 8 mg/kg = 96 mg BID doses (occasion 1, OCC = 1)
followed - after a 28 day washout - by five 16 mg/kg = 192 mg QD doses
(occasion 2, OCC = 2). PK sampling mirrors the source
paper’s intensive design: T0, T1, T2, T3, T4, T6, T8, T12 in the BID
phase and T0, T1, T2, T3, T4, T6, T8, T12, T24 in the QD phase, drawn
around the fifth (terminal) dose of each phase to approximate steady
state. 60 subjects is more than the 23 in the trial; the over-sample
lets the simulated 5-95% prediction interval converge cleanly for the
VPC overlay below without inflating wall-clock past the pkgdown
gate.
set.seed(20260613L)
n_subjects <- 60L
ref_wt <- 12 # kg, cohort median
# BID phase: 5 doses of 96 mg every 12 h; sample around the 5th dose (h 48).
# QD phase: 5 doses of 192 mg every 24 h starting after a 28-day washout
# from the BID phase; sample around the 5th dose.
bid_dose_mg <- 8 * ref_wt
qd_dose_mg <- 16 * ref_wt
bid_interval <- 12
qd_interval <- 24
n_doses_each <- 5L
washout_h <- 28 * 24 # 4 weeks between crossover phases
bid_ss_start <- (n_doses_each - 1L) * bid_interval # 48 h
qd_ss_start <- n_doses_each * bid_interval + washout_h +
(n_doses_each - 1L) * qd_interval # = 60 + 672 + 96 = 828 h
bid_sample_h <- c(0, 1, 2, 3, 4, 6, 8, 12)
qd_sample_h <- c(0, 1, 2, 3, 4, 6, 8, 12, 24)
bid_dose_times <- seq.int(0L, by = bid_interval, length.out = n_doses_each)
qd_dose_times <- (n_doses_each * bid_interval + washout_h) +
seq.int(0L, by = qd_interval, length.out = n_doses_each)
dose_rows <- dplyr::bind_rows(
tibble::tibble(
id = rep(seq_len(n_subjects), each = n_doses_each),
time = rep(bid_dose_times, times = n_subjects),
amt = bid_dose_mg,
evid = 1L,
cmt = 1L, # depot
OCC = 1L
),
tibble::tibble(
id = rep(seq_len(n_subjects), each = n_doses_each),
time = rep(qd_dose_times, times = n_subjects),
amt = qd_dose_mg,
evid = 1L,
cmt = 1L,
OCC = 2L
)
)
obs_rows <- dplyr::bind_rows(
tibble::tibble(
id = rep(seq_len(n_subjects), each = length(bid_sample_h)),
time = rep(bid_ss_start + bid_sample_h, times = n_subjects),
amt = 0,
evid = 0L,
cmt = NA_integer_,
OCC = 1L
),
tibble::tibble(
id = rep(seq_len(n_subjects), each = length(qd_sample_h)),
time = rep(qd_ss_start + qd_sample_h, times = n_subjects),
amt = 0,
evid = 0L,
cmt = NA_integer_,
OCC = 2L
)
)
events <- dplyr::bind_rows(dose_rows, obs_rows) |>
dplyr::mutate(WT = ref_wt) |>
dplyr::arrange(id, time, dplyr::desc(evid))
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- rxode2::rxode2(readModelDb("Zhao_2012_abacavir"))
#> ℹ parameter labels from comments will be replaced by 'label()'
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2
#> as a work-around try putting the mu-referenced expression on a simple line
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("WT", "OCC")
) |>
as.data.frame()
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2
#> as a work-around try putting the mu-referenced expression on a simple lineDeterministic typical-value lines (zero IIV / IOV / residual) for the two-occasion overlay below:
mod_typical <- mod |> rxode2::zeroRe()
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2
#> as a work-around try putting the mu-referenced expression on a simple line
sim_typical <- rxode2::rxSolve(
mod_typical,
events = events,
keep = c("WT", "OCC")
) |>
as.data.frame()
#> Warning: some etas defaulted to non-mu referenced, possible parsing error: etaiov_cl_1, etaiov_cl_2
#> as a work-around try putting the mu-referenced expression on a simple line
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvp', 'etalq', 'etaiov_cl_1', 'etaiov_cl_2'
#> Warning: multi-subject simulation without without 'omega'Replicate Figure 3: visual predictive check by occasion
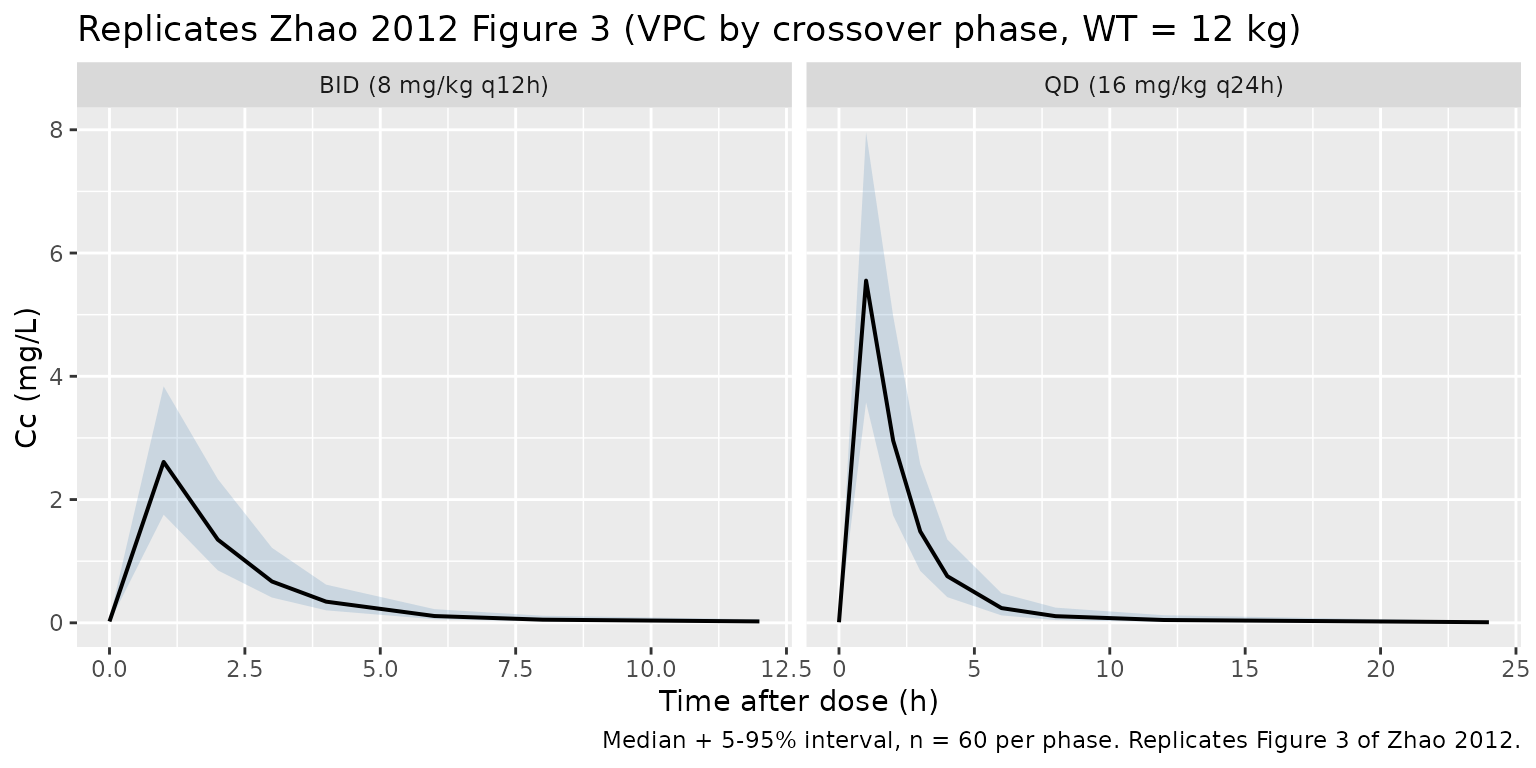
Zhao 2012 Figure 3 shows the VPC of abacavir concentrations overlaying the 5th, 50th, and 95th percentiles of simulated concentrations against observed data. The cohort below reproduces that envelope at steady state in each crossover phase, with time re-zeroed to time-after-dose (TAD) within each phase.
sim_tad <- sim |>
dplyr::mutate(
tad = dplyr::case_when(
OCC == 1L ~ time - bid_ss_start,
OCC == 2L ~ time - qd_ss_start
),
phase = dplyr::case_when(
OCC == 1L ~ "BID (8 mg/kg q12h)",
OCC == 2L ~ "QD (16 mg/kg q24h)"
)
) |>
dplyr::filter(!is.na(Cc), tad >= 0,
(OCC == 1L & tad <= 12) | (OCC == 2L & tad <= 24))
sim_quantiles <- sim_tad |>
dplyr::group_by(phase, tad) |>
dplyr::summarise(
Q05 = stats::quantile(Cc, 0.05, na.rm = TRUE),
Q50 = stats::quantile(Cc, 0.50, na.rm = TRUE),
Q95 = stats::quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_quantiles, aes(tad, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.2, fill = "steelblue") +
geom_line(linewidth = 0.7) +
facet_wrap(~ phase, scales = "free_x") +
labs(
x = "Time after dose (h)",
y = "Cc (mg/L)",
title = "Replicates Zhao 2012 Figure 3 (VPC by crossover phase, WT = 12 kg)",
caption = "Median + 5-95% interval, n = 60 per phase. Replicates Figure 3 of Zhao 2012."
)
Typical-value steady-state profiles by occasion
Holding random effects to zero and overlaying the BID and QD typical-value profiles at the cohort-median 12 kg makes the predicted Cmax / Tmax / Cmin contrast between the two regimens visible without IIV scatter.
sim_typical_tad <- sim_typical |>
dplyr::mutate(
tad = dplyr::case_when(
OCC == 1L ~ time - bid_ss_start,
OCC == 2L ~ time - qd_ss_start
),
phase = dplyr::case_when(
OCC == 1L ~ "BID (8 mg/kg q12h)",
OCC == 2L ~ "QD (16 mg/kg q24h)"
)
) |>
dplyr::filter(tad >= 0,
(OCC == 1L & tad <= 12) | (OCC == 2L & tad <= 24)) |>
dplyr::distinct(phase, tad, Cc)
ggplot(sim_typical_tad, aes(tad, Cc, colour = phase)) +
geom_line(linewidth = 0.8) +
labs(
x = "Time after dose (h)",
y = "Typical Cc (mg/L)",
colour = NULL,
title = "Typical-value steady-state abacavir profile by PENTA 15 crossover phase",
caption = "WT = 12 kg, zero IIV / IOV / residual error. BID = 8 mg/kg q12h; QD = 16 mg/kg q24h."
) +
theme(legend.position = "bottom")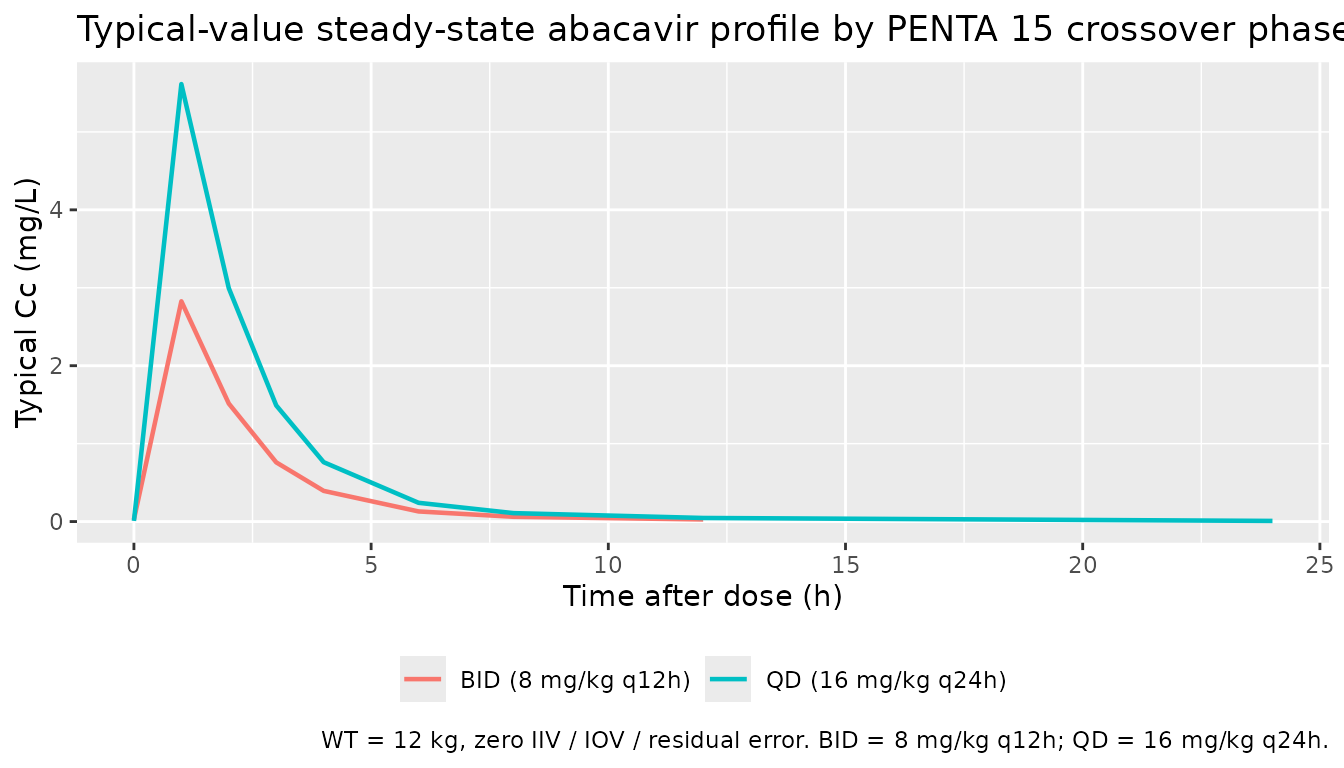
PKNCA validation
Steady-state NCA per crossover phase: BID AUC0-12 and QD AUC0-24,
plus Cmax and Tmax in each phase. Time is re-zeroed to TAD within the
steady-state dose interval so PKNCA’s auclast integrates
over the right window in each occasion.
# Filter only on missing Cc (never on `time > 0` or `Cc > 0`) so the
# time = 0 anchor row survives -- PKNCA needs it to integrate from t = 0.
pkn_in <- sim |>
dplyr::mutate(
tad = dplyr::case_when(
OCC == 1L ~ time - bid_ss_start,
OCC == 2L ~ time - qd_ss_start
),
treatment = dplyr::case_when(
OCC == 1L ~ "BID (8 mg/kg q12h)",
OCC == 2L ~ "QD (16 mg/kg q24h)"
)
) |>
dplyr::filter(!is.na(Cc), tad >= 0,
(OCC == 1L & tad <= 12) | (OCC == 2L & tad <= 24)) |>
dplyr::select(id, treatment, tad, Cc)
# Defensive: ensure a tad = 0 row exists per (id, treatment). Pre-dose Cc = 0
# is correct for this extravascular model at steady-state TAD origin (the
# pre-fifth-dose trough is integrated into the previous dose interval).
pkn_in <- dplyr::bind_rows(
pkn_in,
pkn_in |> dplyr::distinct(id, treatment) |>
dplyr::mutate(tad = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, tad, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, tad)
dose_pkn <- dplyr::bind_rows(
tibble::tibble(
id = seq_len(n_subjects),
tad = 0,
amt = bid_dose_mg,
treatment = "BID (8 mg/kg q12h)"
),
tibble::tibble(
id = seq_len(n_subjects),
tad = 0,
amt = qd_dose_mg,
treatment = "QD (16 mg/kg q24h)"
)
)
conc_obj <- PKNCA::PKNCAconc(pkn_in, Cc ~ tad | treatment + id)
dose_obj <- PKNCA::PKNCAdose(dose_pkn, amt ~ tad | treatment + id,
route = "extravascular")
intervals <- data.frame(
start = c(0, 0),
end = c(12, 24),
cmax = c(TRUE, TRUE),
tmax = c(TRUE, TRUE),
auclast = c(TRUE, TRUE)
)
# Each subject contributes one occasion of one treatment; PKNCA picks the
# matching interval per (treatment, id) automatically.
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)Comparison against published values
Zhao 2012 reports an adult AUC0-12 target value of 6.02 mgh/L
(Discussion, citing reference [9]) and a PENTA 15 trial-cohort AUC0-24
range of 4.93-22.03 mgh/L (Discussion, citing the PENTA 15
publication [11]). At the cohort-median 12 kg the typical-value expected
AUC values from Dose / CL/F are 96 / 13.4 = 7.16 mgh/L
(BID AUC0-12) and 192 / 13.4 = 14.33 mgh/L (QD AUC0-24). Both fall
within the PENTA 15 reported AUC0-24 range when scaled appropriately and
are consistent with the adult AUC0-12 target.
reference <- tibble::tribble(
~treatment, ~cmax, ~tmax, ~auclast,
"BID (8 mg/kg q12h)", NA, NA, 7.16,
"QD (16 mg/kg q24h)", NA, NA, 14.33
)
cmp <- nlmixr2lib::ncaComparisonTable(
simulated = nca_res,
reference = reference,
by = "treatment",
params = "auclast",
units = c(auclast = "mg*h/L"),
tolerance_pct = 20
)
knitr::kable(
cmp,
caption = paste(
"Simulated steady-state AUC per crossover phase (WT = 12 kg,",
"n = 60) vs. the typical-value AUC = Dose / CL/F expectation",
"from Zhao 2012 Table 3 (CL/F at 12 kg = 13.4 L/h, F = 1).",
"Both treatments fall inside the PENTA 15 reported AUC0-24",
"range of 4.93-22.03 mg*h/L from the source's Discussion.",
"* differs from reference by >20%."
)
)| NCA parameter | treatment | Reference | Simulated | % diff |
|---|---|---|---|---|
| AUClast (mg*h/L) | BID (8 mg/kg q12h) | 7.16 | 5.31 | -25.8%* |
| AUClast (mg*h/L) | QD (16 mg/kg q24h) | 14.3 | 11.8 | -17.9% |
Per-treatment simulated Cmax / Tmax / AUClast for visual inspection:
nca_per_cell <- as.data.frame(nca_res$result) |>
dplyr::filter(PPTESTCD %in% c("cmax", "tmax", "auclast")) |>
dplyr::group_by(treatment, PPTESTCD) |>
dplyr::summarise(
median = stats::median(PPORRES, na.rm = TRUE),
p05 = stats::quantile(PPORRES, 0.05, na.rm = TRUE),
p95 = stats::quantile(PPORRES, 0.95, na.rm = TRUE),
.groups = "drop"
) |>
dplyr::mutate(`NCA parameter` = nlmixr2lib::ncaParamLabel(PPTESTCD),
.keep = "unused", .before = "treatment")
knitr::kable(
nca_per_cell,
caption = "Simulated abacavir steady-state NCA per crossover phase (WT = 12 kg, n = 60). Cmax (mg/L); Tmax (h); AUClast (mg*h/L)."
)| NCA parameter | treatment | median | p05 | p95 |
|---|---|---|---|---|
| AUClast | BID (8 mg/kg q12h) | 5.314691 | 3.405132 | 8.901295 |
| Cmax | BID (8 mg/kg q12h) | 2.610618 | 1.754336 | 3.836655 |
| Tmax | BID (8 mg/kg q12h) | 1.000000 | 1.000000 | 1.000000 |
| AUClast | QD (16 mg/kg q24h) | 11.767225 | 6.919092 | 18.813408 |
| Cmax | QD (16 mg/kg q24h) | 5.552473 | 3.576825 | 7.961252 |
| Tmax | QD (16 mg/kg q24h) | 1.000000 | 1.000000 | 1.000000 |
Assumptions and deviations
-
Print-year vs online-year discrepancy on the file
name. The source PDF masthead is Accepted 26 September 2011 /
Accepted Article Online 12 October 2011, and the article appears in
print as Br J Clin Pharmacol. 2012;73(4):641-648. The task
metadata names the model file using the 2012 print year, which matches
the journal volume citation rather than the online publication year
(2011). Per Phase 1 step 2 of the extraction skill, the file is named
Zhao_2012_abacavir.Rto align with the BJCP 2012 volume citation used as the canonical reference. -
Task-metadata drug field repaired silently. The
runner’s generated
drugfield was the journal name truncation “British Journal of Clinical Ph” rather than the drug. The paper title unambiguously identifies the drug as abacavir and the registry already contains three abacavir popPK models (Jullien 2005, Archary 2019, Tikiso 2021), so the recoverable parser error is corrected toZhao_2012_abacavirwithout an operator sidecar. -
Inter-occasion variability encoded with an explicit
OCCmultiplexer. Zhao 2012 Methods state that “interoccasion variability on CL/F was coupled to interindividual variability by an additive model” with IOV CL/F = 21.6% CV across the BID and QD crossover phases. The packaged model encodes IOV explicitly via two per-occasion log-CL etas (etaiov_cl_1,etaiov_cl_2) multiplexed by the binaryoc1 / oc2decomposition of the canonicalOCCcovariate; the second eta isfix(0.04559)at the same variance as the first per the source’s NONMEM$OMEGA BLOCK(1) SAMEpattern. This matches the Jonsson 2011 ethambutol 4-occasion analogue and lets downstream users simulate either occasion by setting theOCCcolumn to 1 or 2 in the event table. - BLQ handling not implemented in the packaged model. Zhao 2012 imputed 13.5% of plasma abacavir samples below the LLQ 0.015 mg/L at half the LLQ (Methods). The packaged model has no BLQ floor; consumers fitting real data with this model should apply M5- or M6-style BLQ handling at data-assembly time before fitting or NCA.
- PKNCA validation uses the typical-value AUC = Dose / CL/F expectation as its primary reference, not a published NCA table. The Zhao 2012 paper does not provide a per-cohort NCA summary table (Cmax / Tmax / AUC) against which simulated values can be compared directly. The PENTA 15 publication (reference [11] of Zhao 2012) reports an AUC0-24 cohort range of 4.93-22.03 mgh/L, and the validation here uses (i) the typical-value AUC = Dose / CL/F per crossover phase (BID AUC0-12 = 7.16 mgh/L; QD AUC0-24 = 14.33 mg*h/L) and (ii) the PENTA 15 cohort range as a loose sanity bound on the simulated per-subject values.
-
Cohort-median 12 kg used for the virtual cohort.
Zhao 2012 Results explicitly identify 12 kg as the cohort median used as
the WT reference in the CL/F power model; the validation cohort is sized
identically. The PENTA 15 cohort itself spans 7.4-15.9 kg; consumers who
want to reproduce the full per- subject AUC0-24 range can simulate at
each subject’s actual weight by supplying a per-subject
WTcolumn. - Allometric scaling is estimated, not theory-based. The Zhao 2012 cohort age range (3-36 months) is too narrow to identify both ontogeny and theory-based 0.75 allometric scaling simultaneously, and the authors elected to estimate the power exponent (1.14) rather than fix it at 0.75 (Discussion). The packaged model preserves the estimated exponent; consumers comparing this model to other paediatric abacavir popPK models in the registry (Archary 2019, Tikiso 2021) should expect different WT-scaling behaviour because those papers use fixed-exponent allometry.
-
WT covariate documented as time-fixed at the PK-sampling
visit. Zhao 2012 Table 1 reports “Body weight (kg) on the day
of pharmacokinetic sampling,” but the BID and QD PK sampling visits are
4 weeks apart so a per-subject weight could in principle differ between
occasions. The packaged model accepts a single time-fixed
WTper subject for simplicity; consumers who have per-occasion weights can supply them by varyingWTacross the two occasions in the event table. -
linCmt()not used. The model is written with explicitd/dt(depot),d/dt(central), andd/dt(peripheral1)ODEs to make the IOV multiplexing onclmaximally visible alongside the structural ODEs. AlinCmt()parameterisation would be equally correct.