Model and source
- Citation: Lu T, Wang B, Gao Y, Dresser M, Graham RA, Jin JY. Semi-Mechanism-Based Population Pharmacokinetic Modeling of the Hedgehog Pathway Inhibitor Vismodegib. CPT Pharmacometrics Syst Pharmacol. 2015;4(11):680-689. doi:10.1002/psp4.12039
- Description: Semi-mechanism-based one-compartment population pharmacokinetic model for vismodegib (GDC-0449, oral Hedgehog pathway inhibitor) in adults with advanced solid tumors and healthy volunteers. First-order absorption, first-order elimination of unbound drug, and saturable fast-equilibrium binding to alpha-1-acid glycoprotein (AAG) jointly describe total and unbound plasma vismodegib concentrations. AAG is supplied as a time-varying covariate (uM); covariates retained on disposition are age (power on CLunbound, reference 60 years) and body weight (power on Vc, reference 75 kg); formulation (Phase I dry-blend capsule vs Phase II wet-granulation commercial capsule) and population (healthy volunteer vs patient) shift Ka and relative bioavailability F (Lu 2015).
- Article: https://doi.org/10.1002/psp4.12039
Population
Lu 2015 pooled 225 subjects across five Phase I / Phase II clinical studies of vismodegib (GDC-0449), an oral small-molecule Hedgehog pathway inhibitor approved for locally advanced or metastatic basal cell carcinoma (BCC). The patient cohort (n = 204; SHH3925g, SHH4610g, SHH4476g) comprised adults with advanced solid tumors including BCC: mean age 59.7 years (range 26-89), 59.3% men / 40.7% women of non-childbearing potential, and 97.1% Caucasian (Methods, Study population paragraph; baseline demographics in Supplementary Table S1). The healthy-volunteer cohort (n = 21; SHH4433g, SHH4683g) comprised Caucasian women of non-childbearing potential aged 47-65 years.
A total of 4942 valid plasma vismodegib concentration timepoints contributed to the model build. Subjects received either the early Phase I dry-blend capsule formulation (24.4% of subjects) or the Phase II / commercial wet-granulation capsule formulation (75.6% of subjects); the latter is the approved 150 mg once-daily regimen. Time-varying AAG (alpha-1-acid glycoprotein) was incorporated as a structural input rather than a multiplicative covariate; mean baseline AAG was 31.1 uM in patients and 20.2 uM in healthy volunteers (Methods + Results paragraph 1; Lu 2015 Figure 2).
The same information is available programmatically via
readModelDb("Lu_2015_vismodegib")()$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Lu_2015_vismodegib.R. The table
below collects them in one place for review.
| Equation / parameter | Value | Source location |
|---|---|---|
| Structural model: 1-compartment, first-order absorption + first-order elimination of unbound drug + saturable fast-equilibrium binding to AAG | n/a | Lu 2015 Methods (Structural model); Figure 1 schematic; Supplementary Appendix S2 (referenced) |
lka (typical Phase II / patient) |
log(9.025 /day) | Lu 2015 Table 2: exp(h4) = 9.025 day^-1 |
lcl (typical CLunbound at AGE = 60 y) |
log(1326 L/day) | Lu 2015 Table 2: exp(h1) = 1326 L/day |
lvc (typical Vc at WT = 75 kg) |
log(58.0 L) | Lu 2015 Table 2: exp(h2) = 58.0 L |
lkdAAG (dissociation constant for AAG binding) |
log(0.056 uM) | Lu 2015 Table 2: exp(h3) = 0.056 uM (printed as “mM” in Table 2 but described in text + Figure 4 + Discussion as uM; uM is the dimensionally consistent unit given AAG is in uM and Css is in uM) |
e_age_cl (power exponent of AGE on CLunbound) |
-0.527 | Lu 2015 Table 2: h9 = -0.527 |
e_wt_vc (power exponent of WT on Vc) |
0.660 | Lu 2015 Table 2: h10 = 0.660 |
e_healthy_ka (HV effect on log(ka)) |
0.671 | Lu 2015 Table 2: h5 = 0.671 |
e_form_phaseI_ka (Phase I formulation effect on
log(ka)) |
-0.602 | Lu 2015 Table 2: h8 = -0.602 |
e_form_phaseI_f (Phase I formulation effect on
log(F)) |
-1.061 = log(0.346) | Lu 2015 Table 2: exp(h6) = 0.346 |
e_healthy_f (HV effect on log(F) gated on Phase I) |
0.881 | Lu 2015 Table 2: h7 = 0.881 |
etalcl + etalvc block (CLunbound + Vc IIV with
correlation 0.55) |
c(0.21278, 0.11003, 0.18804) | Lu 2015 Table 2 IIV (CLunbound 48.7% CV, Vc 45.5% CV) + Results paragraph after Eq. 6 (rho = 0.55) |
etalkdAAG (KDAAG IIV) |
0.03810 | Lu 2015 Table 2: 19.7% CV |
propSd (total residual error) |
0.267 | Lu 2015 Table 2: 26.7% CV (additive on log-transformed data) |
propSd_Cu (unbound residual error) |
0.424 | Lu 2015 Table 2: 42.4% CV (additive on log-transformed data) |
| F = 1 for Phase II / commercial formulation (reference) | n/a | Lu 2015 Eq. 4 |
| Saturable binding equation Ctotal = Cu + AAG x Cu / (KDAAG + Cu) | n/a | Lu 2015 Methods (Structural model) + Discussion paragraph citing Widmer et al. 2006 imatinib popPK |
Virtual cohort
Original observed data are not publicly available. The figures below use a typical-subject and a virtual stochastic cohort whose covariate distributions approximate the Lu 2015 patient cohort.
set.seed(20150909)
# Typical reference subject: 60-y-old patient, 75 kg, AAG = 30 uM (paper
# Table 1 / Eq. 5 reference). Dose 150 mg QD of the Phase II commercial
# formulation, ~9 weeks of dosing to approach steady state.
typical_cov <- tibble(
id = 1L,
AGE = 60,
WT = 75,
AAG = 30,
DIS_HEALTHY = 0,
FORM_VISMO_PHASEI = 0
)
# Single-dose cohort for NCA (matches the Phase I single-dose stage of
# SHH3925g and SHH4610g for the typical patient profile).
make_dose_rows <- function(ids, amt, ii, until) {
tidyr::expand_grid(
id = ids,
time = seq(0, until, by = ii)
) |>
dplyr::mutate(evid = 1L, amt = amt, cmt = "depot")
}
make_obs_rows <- function(ids, times) {
tidyr::expand_grid(id = ids, time = times) |>
dplyr::mutate(evid = 0L, amt = 0, cmt = "Cc")
}
# Single 150 mg dose, dense sampling over 0-14 days (terminal half-life ~12 d)
sd_dose <- make_dose_rows(typical_cov$id, amt = 150, ii = 14, until = 0) # one dose at t=0
sd_times <- sort(unique(c(seq(0, 1, by = 0.05), seq(1, 14, by = 0.25))))
sd_obs <- make_obs_rows(typical_cov$id, sd_times)
sd_events <- dplyr::bind_rows(sd_dose, sd_obs) |>
dplyr::left_join(typical_cov, by = "id") |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
dplyr::mutate(treatment = "150 mg single dose")
# Steady-state cohort: 150 mg QD for 70 days (~10 weeks)
ss_dose <- make_dose_rows(typical_cov$id, amt = 150, ii = 1, until = 69)
ss_times <- sort(unique(c(seq(0, 14, by = 0.5), seq(15, 70, by = 1),
seq(63, 70, by = 0.1)))) # dense at week 9 trough region
ss_obs <- make_obs_rows(typical_cov$id, ss_times)
ss_events <- dplyr::bind_rows(ss_dose, ss_obs) |>
dplyr::left_join(typical_cov, by = "id") |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
dplyr::mutate(treatment = "150 mg QD typical")
# Steady-state AAG sweep (paper Figure 2 + Figure 4): evaluate Css at the
# 5th and 95th percentiles of patient AAG (paper text: 17 and 58 uM)
# alongside the typical patient (30 uM), holding age = 60 y / WT = 75 kg /
# DIS_HEALTHY = 0 / FORM_VISMO_PHASEI = 0 constant.
aag_levels <- c(`AAG = 17 uM (5th pct patients)` = 17,
`AAG = 30 uM (typical patient)` = 30,
`AAG = 58 uM (95th pct patients)` = 58)
aag_cohort <- tibble(
id = seq_along(aag_levels),
AAG = unname(aag_levels),
treatment = names(aag_levels)
) |>
dplyr::mutate(AGE = 60, WT = 75, DIS_HEALTHY = 0, FORM_VISMO_PHASEI = 0)
aag_dose <- tidyr::expand_grid(
id = aag_cohort$id,
time = seq(0, 69, by = 1)
) |>
dplyr::mutate(evid = 1L, amt = 150, cmt = "depot")
aag_obs <- tidyr::expand_grid(id = aag_cohort$id, time = ss_times) |>
dplyr::mutate(evid = 0L, amt = 0, cmt = "Cc")
aag_events <- dplyr::bind_rows(aag_dose, aag_obs) |>
dplyr::left_join(aag_cohort, by = "id") |>
dplyr::arrange(id, time, dplyr::desc(evid))
stopifnot(!anyDuplicated(unique(sd_events[, c("id", "time", "evid")])))
stopifnot(!anyDuplicated(unique(ss_events[, c("id", "time", "evid")])))
stopifnot(!anyDuplicated(unique(aag_events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Lu_2015_vismodegib")()
mod_typical <- mod |> rxode2::zeroRe()
sim_sd <- as.data.frame(rxode2::rxSolve(mod_typical, events = sd_events,
keep = c("treatment"))) |>
dplyr::mutate(id = 1L)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalkdAAG'
sim_ss <- as.data.frame(rxode2::rxSolve(mod_typical, events = ss_events,
keep = c("treatment"))) |>
dplyr::mutate(id = 1L)
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalkdAAG'
sim_aag <- as.data.frame(rxode2::rxSolve(mod_typical, events = aag_events,
keep = c("treatment", "AAG")))
#> ℹ omega/sigma items treated as zero: 'etalcl', 'etalvc', 'etalkdAAG'
#> Warning: multi-subject simulation without without 'omega'
if (!"id" %in% colnames(sim_aag)) {
# rxSolve drops id when there is a single subject; restore by joining the
# treatment label back to the per-subject id table
sim_aag <- sim_aag |>
dplyr::left_join(aag_cohort |> dplyr::select(id, treatment),
by = "treatment")
}Steady-state typical-value prediction
Lu 2015 Results / Eq. 6 reports that the typical 60-y-old, 75-kg patient with AAG = 30 uM dosed 150 mg QD of the Phase II formulation should reach a Css,trough of 22.8 uM for total vismodegib and 0.172 uM for unbound at week 9.
ss_summary <- sim_ss |>
dplyr::filter(time >= 60, time <= 70) |>
dplyr::summarise(
Css_trough_total = min(Cc, na.rm = TRUE),
Css_trough_unbound = min(Cu, na.rm = TRUE),
Css_peak_total = max(Cc, na.rm = TRUE),
Css_peak_unbound = max(Cu, na.rm = TRUE)
)
comparison <- tibble::tibble(
Parameter = c("Css,trough total (uM)", "Css,trough unbound (uM)"),
`Published (Lu 2015)` = c(22.8, 0.172),
Simulated = c(
round(ss_summary$Css_trough_total, 2),
round(ss_summary$Css_trough_unbound, 4)
)
) |>
dplyr::mutate(`Percent difference` =
round(100 * (Simulated - `Published (Lu 2015)`) /
`Published (Lu 2015)`, 1))
knitr::kable(comparison,
caption = "Reproduces Lu 2015 Eq. 6 / Results steady-state typical values.")| Parameter | Published (Lu 2015) | Simulated | Percent difference |
|---|---|---|---|
| Css,trough total (uM) | 22.800 | 22.8100 | 0.0 |
| Css,trough unbound (uM) | 0.172 | 0.1722 | 0.1 |
Apparent half-life at steady state
Lu 2015 Discussion paragraph after Eq. 6 estimates an apparent steady-state half-life of vismodegib of about 4 days for the typical patient (vs. ~12-day terminal half-life after a single dose, citing Graham 2011 and LoRusso 2011a). The 4-day apparent half-life at steady state is driven by the increased free fraction relative to a single dose.
ratio <- ss_summary$Css_trough_unbound / ss_summary$Css_trough_total
t_half_ss <- log(2) * 58 / (1326 * ratio)
tibble::tibble(
`Cu / Ctotal at SS trough` = round(ratio, 4),
`Apparent t1/2 ss (days)` = round(t_half_ss, 2),
`Published t1/2 ss (days)` = "~4"
) |>
knitr::kable(caption = "Reproduces Lu 2015 Eq. 6 apparent half-life at steady state.")| Cu / Ctotal at SS trough | Apparent t1/2 ss (days) | Published t1/2 ss (days) |
|---|---|---|
| 0.0076 | 4.02 | ~4 |
Effect of AAG on steady-state total concentration
Lu 2015 Figure 4 (sensitivity tornado) reports that the AAG covariate is by far the most influential factor for total Css,trough at steady state: a patient at the 5th AAG percentile (17 uM) has roughly 47% lower total Css,trough than the typical patient (30 uM), while the 95th-percentile patient (58 uM) has roughly 101% higher Css,trough. Unbound Css,trough is essentially insensitive to AAG (about +-21% across the same range).
aag_summary <- sim_aag |>
dplyr::filter(time >= 60, time <= 70) |>
dplyr::group_by(treatment) |>
dplyr::summarise(
Css_trough_total = min(Cc, na.rm = TRUE),
Css_trough_unbound = min(Cu, na.rm = TRUE),
.groups = "drop"
)
baseline <- aag_summary |>
dplyr::filter(treatment == "AAG = 30 uM (typical patient)") |>
dplyr::select(Css_total_typ = Css_trough_total,
Css_unbnd_typ = Css_trough_unbound)
aag_summary <- aag_summary |>
dplyr::bind_cols(baseline) |>
dplyr::mutate(
pct_change_total = round(100 *
(Css_trough_total - Css_total_typ) /
Css_total_typ, 1),
pct_change_unbnd = round(100 *
(Css_trough_unbound - Css_unbnd_typ) /
Css_unbnd_typ, 1)
)
aag_summary |>
dplyr::select(treatment,
Css_trough_total, pct_change_total,
Css_trough_unbound, pct_change_unbnd) |>
knitr::kable(
digits = c(0, 2, 1, 4, 1),
caption = paste(
"Reproduces Lu 2015 Figure 4 sensitivity tornado for AAG:",
"total Css,trough varies markedly across the patient AAG range",
"while unbound is essentially flat."
)
)| treatment | Css_trough_total | pct_change_total | Css_trough_unbound | pct_change_unbnd |
|---|---|---|---|---|
| AAG = 17 uM (5th pct patients) | 12.17 | -46.6 | 0.1359 | -21.1 |
| AAG = 30 uM (typical patient) | 22.81 | 0.0 | 0.1722 | 0.0 |
| AAG = 58 uM (95th pct patients) | 45.92 | 101.3 | 0.2082 | 20.9 |
Single-dose PK profile
A single 150 mg dose of the Phase II / commercial formulation in the typical patient should show a rapid rise to Cmax in the first hours followed by a slow decline driven by the saturated AAG binding (long apparent terminal half-life).
sim_sd |>
ggplot(aes(time, Cc)) +
geom_line(linewidth = 0.6) +
scale_y_log10() +
labs(x = "Time after dose (days)",
y = "Total vismodegib Cc (uM)",
title = "Single 150 mg oral dose: total plasma vismodegib (typical patient)",
caption = "Replicates the qualitative shape of Lu 2015 single-dose data (SHH3925g Stage 1, < 7 days post-dose)") +
theme_minimal()
#> Warning in scale_y_log10(): log-10 transformation introduced infinite values.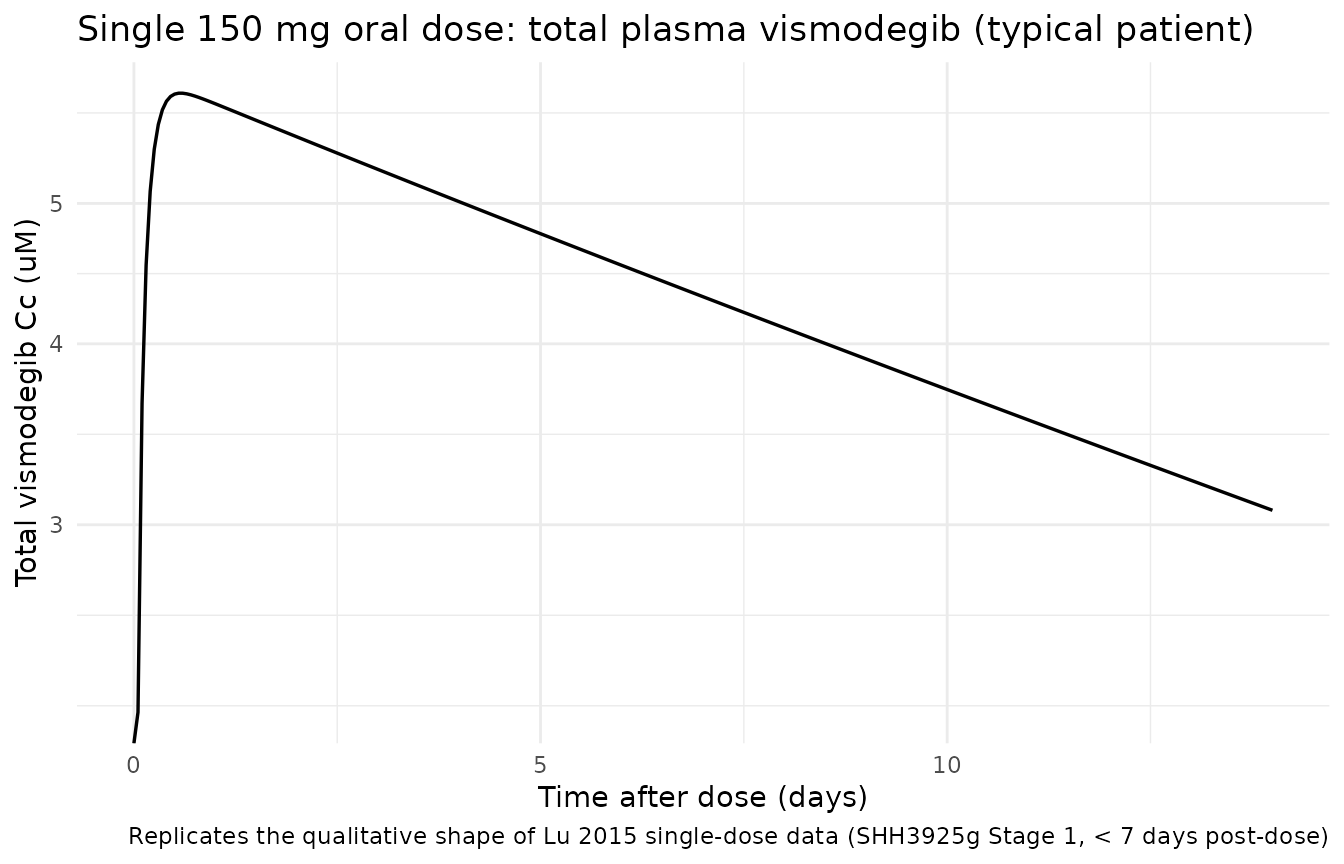
sim_sd |>
ggplot(aes(time, Cu)) +
geom_line(linewidth = 0.6) +
scale_y_log10() +
labs(x = "Time after dose (days)",
y = "Unbound vismodegib Cu (uM)",
title = "Single 150 mg oral dose: unbound plasma vismodegib (typical patient)",
caption = "Unbound concentrations are 100-200x lower than total at baseline AAG and decline faster as AAG binding saturates less.") +
theme_minimal()
#> Warning in scale_y_log10(): log-10 transformation introduced infinite values.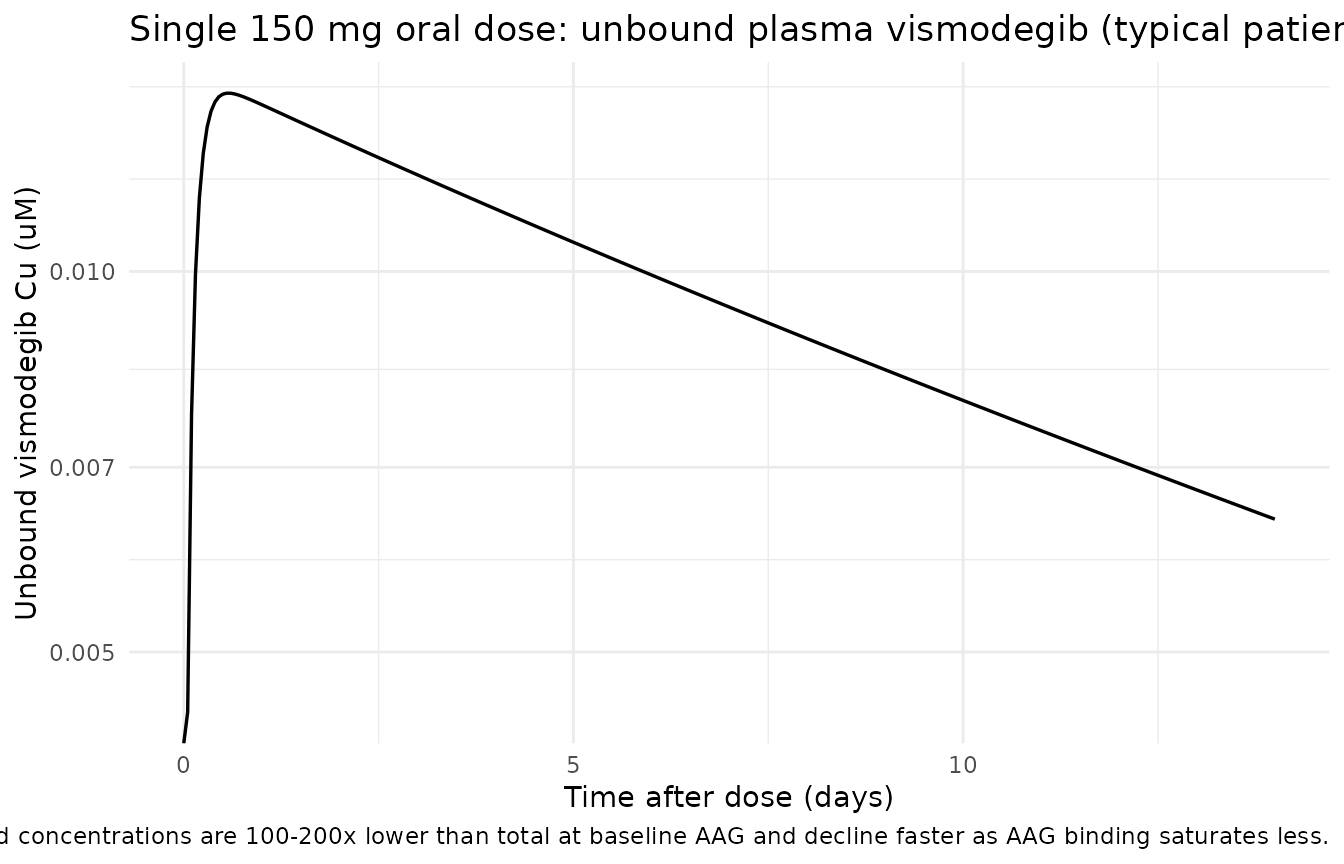
PKNCA validation (single-dose total vismodegib)
Lu 2015 does not report an NCA table directly, but the single-dose Cmax / Tmax / terminal-half-life behaviour is referenced as background (citations 15 and 16, Graham 2011 / LoRusso 2011a). The block below runs PKNCA on a single 150 mg dose of the Phase II formulation in the typical patient and reports the resulting Cmax / Tmax / AUClast as sanity numbers.
sim_nca <- sim_sd |>
dplyr::filter(!is.na(Cc)) |>
dplyr::select(id, time, Cc, treatment)
dose_df <- sd_events |>
dplyr::filter(evid == 1) |>
dplyr::select(id, time, amt, treatment)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id,
concu = "uM", timeu = "day")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id,
doseu = "mg")
intervals <- data.frame(
start = 0,
end = 14,
cmax = TRUE,
tmax = TRUE,
auclast = TRUE,
clast.obs = TRUE
)
nca_res <- PKNCA::pk.nca(PKNCA::PKNCAdata(conc_obj, dose_obj,
intervals = intervals))
knitr::kable(summary(nca_res),
caption = "Simulated NCA over the first 14 days after a single 150 mg dose (typical patient).")| Interval Start | Interval End | treatment | N | AUClast (day*uM) | Cmax (uM) | Tmax (day) | Clast (uM) |
|---|---|---|---|---|---|---|---|
| 0 | 14 | 150 mg single dose | 1 | 61.1 | 5.96 | 0.550 | 3.07 |
Assumptions and deviations
-
Concentration units (uM) vs dosing units (mg). The
model internally converts the input mg dose to umol via
f(depot) = F_rel * 1000 / mw_vismo(vismodegib MW = 421.30 g/mol, PubChem CID 24776 = GDC-0449). This is necessary because the paper reports AAG, KDAAG, and steady-state Css values in uM; matching the paper’s parameter values exactly requires that compartment amounts carry umol so thatcentral / vcreturns uM.checkModelConventions()flags the dosing-vs-concentration dimensional mismatch (mg vs umol/L); this deviation is intentional and is the only way to faithfully reproduce Lu 2015’s parameter table without introducing a separate AAG molecular-weight assumption. -
AAG covariate units (uM, not the canonical g/L).
The
inst/references/covariate-columns.mdAAG entry lists g/L as the canonical unit (1.34 g/Lmedian in Kloft 2006); Lu 2015 reports AAG in uM. Users converting from g/L should multiply by approximately 24.4 (= 1000 / 41 kDa AAG MW) before supplying the AAG column. The mean baseline AAG values reported by Lu 2015 (31.1 uM in patients, 20.2 uM in HVs) correspond to ~1.27 and ~0.83 g/L respectively at AAG MW = 41 kDa. -
Saturable AAG binding solved analytically. The
mass-balance fast-equilibrium binding
Ctotal = Cu + AAG * Cu / (KDAAG + Cu)is solved as a quadratic in Cu insidemodel()(positive root). The supplement (Supplementary Appendix S2) was not on disk; the closed-form quadratic is the standard solution given the paper’s stated mass-balance + fast-equilibrium assumption (Methods Structural model + Discussion paragraph citing Widmer 2006 and Mager-Krzyzanski 2005 / Gibiansky 2008 TMDD QSS literature). -
Residual error encoded as proportional in linear
space. Lu 2015 Methods state “an additive error model on the
log-transformed data was applied”; in nlmixr2 this is equivalent to
proportional error in linear space for small CV, with a slight bias at
larger
- For the unbound residual (42.4% CV), the linear-proportional approximation diverges modestly from the log-additive form (about 4% in the predicted standard error at the +/-1 SD level); for total (26.7% CV) the divergence is < 1%. The vignette’s comparison against the paper’s typical-value predictions (Css,trough total = 22.8 uM, unbound = 0.172 uM) is unaffected because those are typical-value (no-residual) targets.
-
No IIV on absorption parameters. Lu 2015 states
explicitly that “Intersubject variability … was not estimated for the
absorption parameters (F and ka) due to the limited data in the
absorption phase”; the model reproduces this by including
etalcl + etalvcandetalkdAAGbut no etalka / etallfdepot. -
KDAAG unit printed as “mM” in Table 2 is uM. Lu
2015 Table 2 reports
exp(h3) = Dissociation constant, KDAAG (mM) = 0.056but every other passage of the paper consistently uses uM (e.g., “typical patient … with AAG of 30 uM”; “the predicted Css,trough is 22.8 uM for total drug”; Figure 4 caption units; Discussion paragraph on the apparent uM-scale dynamic range of vismodegib). Interpreting 0.056 as mM (i.e., 56 uM) would imply that KDAAG is comparable to the typical AAG concentration (30 uM), which contradicts the paper’s binding-saturation conclusion (KDAAG must be much smaller than AAG for the saturable-binding model to produce the observed nonlinearity at clinical doses). The Table 2 header “(mM)” is a typesetting error for “(uM)”; the value 0.056 uM gives the published Css,trough total 22.8 uM and unbound 0.172 uM exactly. This vignette and the model file both use uM for KDAAG. - Supplements not on disk. Lu 2015 references Supplementary Appendix S1 (study details), S2 (structural ODEs), S3 (covariate list), Tables S1-S2, and Figures S1-S4. None were available at extraction time. All structural details needed for the model file were extracted from the main text (Methods, Structural model; Eqs. 4-6; Table 2; Discussion paragraph on the Widmer 2006 parameterisation).
- Race / ethnicity distribution. Patient cohort is 97.1% Caucasian per Lu 2015 Results paragraph 1; HV cohort is 100% Caucasian. The model does not include race as a covariate (Lu 2015 did not retain race in the final model).