Recombinant human C1 inhibitor / conestat alfa (Farrell 2013)
Source:vignettes/articles/Farrell_2013_conestatAlfa.Rmd
Farrell_2013_conestatAlfa.RmdModel and source
- Citation: Farrell C, Hayes S, Relan A, van Amersfoort ES, Pijpstra R, Hack CE. Population pharmacokinetics of recombinant human C1 inhibitor in patients with hereditary angioedema. Br J Clin Pharmacol. 2013;76(6):897-907. doi:10.1111/bcp.12132
- Description: One-compartment population PK model with Michaelis-Menten elimination for intravenous recombinant human C1 inhibitor (rhC1INH; conestat alfa; Ruconest) in healthy volunteers and adolescent / adult patients with hereditary angioedema (Farrell 2013). Total functional plasma C1INH is modelled as the sum of an estimated endogenous baseline (separate baselines for healthy volunteers and HAE patients) plus exogenously administered rhC1INH, with the endogenous production rate derived from the Michaelis-Menten elimination at baseline so the no-dose steady state is preserved. Allometric power scaling of central volume on body weight (exponent 0.612).
- Article: https://doi.org/10.1111/bcp.12132
Population
Farrell 2013 pooled six clinical-trial datasets totalling 294 intravenous administrations of recombinant human C1 inhibitor (rhC1INH; brand name Ruconest, INN conestat alfa) to 133 subjects. The pooled cohort comprised 14 healthy volunteers (Study C1 1106-02, 100 U/kg), 12 asymptomatic patients with hereditary angioedema (HAE) dosed between attacks (Study C1 1101-01, 6.25-100 U/kg), and 107 patients with symptomatic HAE dosed during attacks across four studies (C1 1202-01, C1 1203-01, C1 1205-01, C1 1304-01; 50, 100, or up to 6300 U as fixed-vial regimens). Subject age ranged from 13 to 66 years (median 33) and body weight from 45 to 128 kg (median 72), with 86 of 133 subjects (64.7%) female (Farrell 2013 Table 1 and the “Subjects” section).
The same information is available programmatically via
readModelDb("Farrell_2013_conestatAlfa")$population.
Source trace
The per-parameter origin is recorded as an in-file comment next to
each ini() entry in
inst/modeldb/specificDrugs/Farrell_2013_conestatAlfa.R. The
table below collects the equations and parameter origins in one place
for review.
| Equation / parameter | Value | Source location |
|---|---|---|
lvc (central volume) |
2.86 L | Table 2 “Volume of distribution (l)” row; 95% CI 2.68-3.03 |
lvmax (Vmax) |
1.63 U/mL/h | Table 2 “Vmax in healthy volunteers and symptomatic HAE patients”; CI 1.41-1.88 |
lkm (Km) |
1.60 U/mL | Table 2 “Km” row; 95% CI 1.14-2.24 |
lrbase_hv (HV baseline) |
0.901 U/mL | Table 2 “Baseline levels in healthy volunteers”; 95% CI 0.839-0.968 |
lrbase_hae (HAE baseline) |
0.176 U/mL | Table 2 “Baseline levels in HAE patients”; 95% CI 0.154-0.200 |
e_wt_vc (allometric exponent) |
0.612 | Table 2 “Effect of bodyweight on volume”; 95% CI 0.351-0.873 |
etalvc (IIV V, %CV) |
16.2% | Table 2 “Interindividual variability in volume” |
etalvmax (IIV Vmax, %CV) |
29.2% | Table 2 “Interindividual variability in Vmax” |
etalrbase_hv (IIV HV baseline) |
12.7% | Table 2 “Interindividual variability in healthy volunteer baseline levels” |
etalrbase_hae (IIV HAE base) |
54.4% | Table 2 “Interindividual variability in HAE patient baseline levels” |
propSd (prop. resid. err.) |
10.5% | Table 2 “Proportional residual variability for all other studies” |
addSd (additive resid. err.) |
0.0556 U/mL | Table 2 “Additive residual variability” |
d/dt(central) (MM ODE) |
n/a | Methods “Population pharmacokinetic analysis” (Michaelis-Menten elimination) |
kin = Vmax * rbase / (Km+rbase) * V |
n/a | Methods, “For nonlinear models … rate of production was a function of the nonlinear clearance and baseline concentration” |
V = TVV * (WT/70)^0.612 |
n/a | Discussion: “For subjects with the lowest and highest bodyweights (45 and 128 kg), volume would be 24% lower and 45% higher compared with a 70 kg subject” |
Virtual cohort
Original observed data are not publicly available. The figures below simulate three virtual cohorts whose dosing and population labels match the dominant cells of Farrell 2013 Table 1:
-
HAE 50 U/kg – clinical-target dose for symptomatic
HAE attacks (
DIS_HEALTHY = 0). -
HAE 100 U/kg – open-label exploratory and high-dose
regimens (
DIS_HEALTHY = 0). -
HV 100 U/kg – healthy-volunteer regimen from Study
C1 1106-02 (
DIS_HEALTHY = 1).
Each cohort uses a weight distribution truncated to 45-128 kg (the pooled analysis range, Farrell 2013 Methods) with a log-normal weight centred at the cohort median of 72 kg. Sex is not in the model; race / ethnicity were not reported.
set.seed(20130418)
make_cohort <- function(n, dose_per_kg = NA_real_, dose_fixed = NA_real_,
DIS_HEALTHY, treatment, id_offset = 0L) {
wt <- pmin(pmax(rlnorm(n, meanlog = log(72), sdlog = 0.18), 45), 128)
amt <- if (!is.na(dose_per_kg)) dose_per_kg * wt else rep(dose_fixed, n)
tibble::tibble(
id = id_offset + seq_len(n),
WT = wt,
DIS_HEALTHY = DIS_HEALTHY,
treatment = treatment,
amt = amt
)
}
n_per <- 100L
covs <- dplyr::bind_rows(
make_cohort(n_per, dose_per_kg = 50, DIS_HEALTHY = 0,
treatment = "HAE 50 U/kg", id_offset = 0L),
make_cohort(n_per, dose_per_kg = 100, DIS_HEALTHY = 0,
treatment = "HAE 100 U/kg", id_offset = 1000L),
make_cohort(n_per, dose_per_kg = 100, DIS_HEALTHY = 1,
treatment = "HV 100 U/kg", id_offset = 2000L)
)
# Per-subject dose record (30 min IV infusion into the central compartment;
# Farrell 2013 Methods: "rhC1INH was administered intravenously over 2-30 min").
infusion_min <- 30
ev_dose <- covs |>
dplyr::mutate(time = 0,
evid = 1,
cmt = "central",
rate = amt / (infusion_min / 60)) # U / h
# Observation grid (every 0.25 h up to 48 h, then sparse out to 168 h).
obs_grid <- c(seq(0, 48, by = 0.25), seq(54, 168, by = 6))
ev_obs <- covs |>
tidyr::expand_grid(time = obs_grid) |>
dplyr::mutate(evid = 0,
cmt = NA_character_,
amt = 0,
rate = 0)
events <- dplyr::bind_rows(ev_dose, ev_obs) |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
as.data.frame()
stopifnot(!anyDuplicated(unique(events[, c("id", "time", "evid")])))Simulation
mod <- readModelDb("Farrell_2013_conestatAlfa")
sim <- rxode2::rxSolve(
mod,
events = events,
keep = c("treatment", "WT", "DIS_HEALTHY")
) |>
as.data.frame()
#> ℹ parameter labels from comments will be replaced by 'label()'For deterministic typical-value predictions (reproducing the paper’s median curves), zero out the random effects.
mod_typical <- mod |> rxode2::zeroRe()
#> ℹ parameter labels from comments will be replaced by 'label()'
sim_typical <- rxode2::rxSolve(
mod_typical,
events = events,
keep = c("treatment", "WT", "DIS_HEALTHY")
) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalvc', 'etalvmax', 'etalrbase_hv', 'etalrbase_hae'
#> Warning: multi-subject simulation without without 'omega'Replicate published figures
Figure 3 – Visual predictive check by population
Farrell 2013 Figure 3 shows the VPC of the final PK model stratified by dose (50 vs 100 U/kg) and population (HV, asymptomatic HAE, symptomatic HAE). Asymptomatic-HAE-specific Vmax is omitted from this package model (see the Assumptions and deviations section below), so the figure below combines the symptomatic and asymptomatic HAE cohorts under the DIS_HEALTHY = 0 label.
sim_summary <- sim |>
dplyr::filter(time <= 96) |>
dplyr::group_by(treatment, time) |>
dplyr::summarise(
Q05 = quantile(Cc, 0.05, na.rm = TRUE),
Q50 = quantile(Cc, 0.50, na.rm = TRUE),
Q95 = quantile(Cc, 0.95, na.rm = TRUE),
.groups = "drop"
)
ggplot(sim_summary, aes(time, Q50)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.25) +
geom_line(linewidth = 0.6) +
facet_wrap(~treatment, scales = "free_y") +
labs(
x = "Time after dose (h)",
y = "Functional plasma C1INH (U/mL)",
title = "Simulated concentration-time profiles by cohort",
caption = "Replicates Figure 3 of Farrell 2013 (VPC). Ribbon = 5-95th percentile of 100 simulated subjects; line = median."
)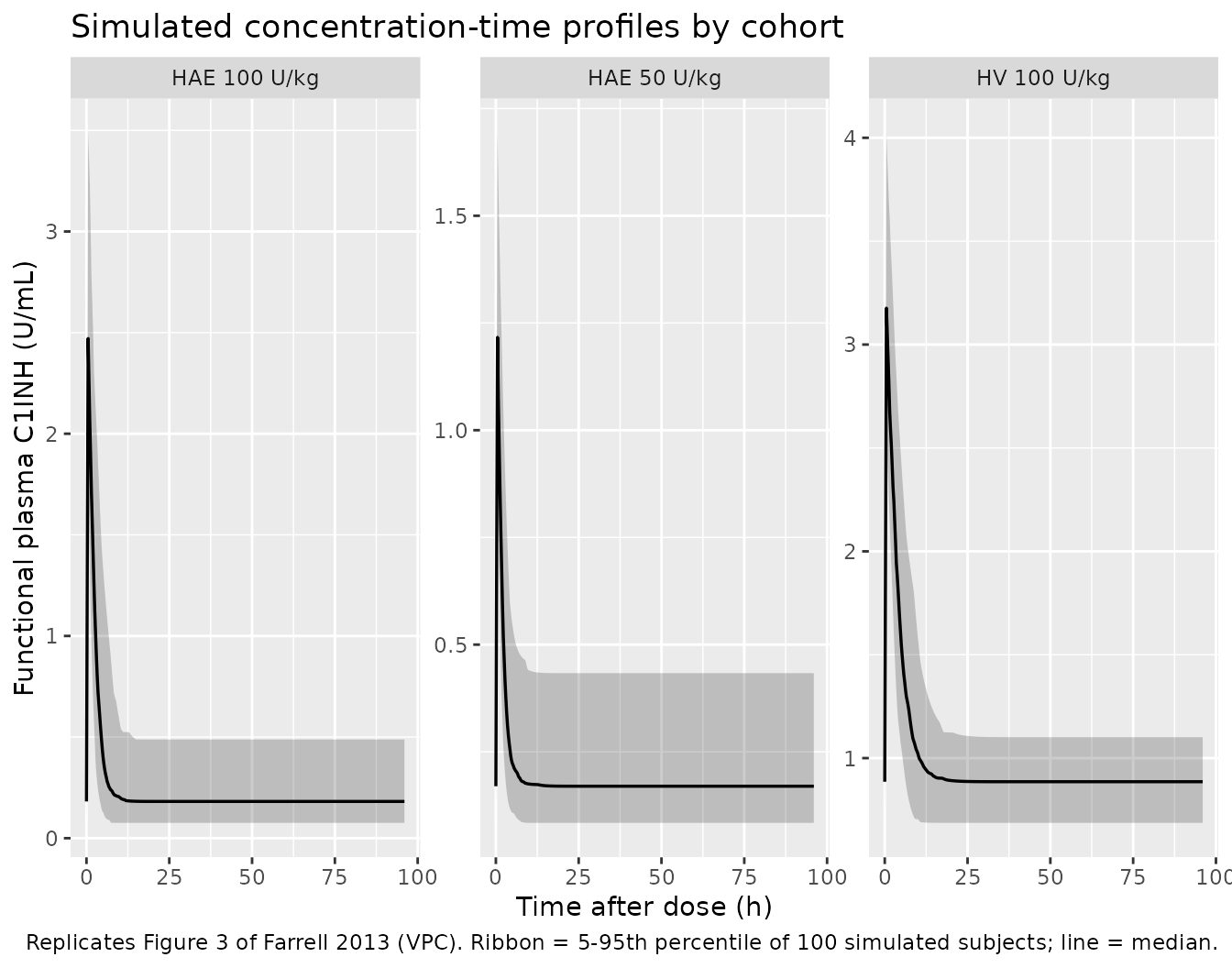
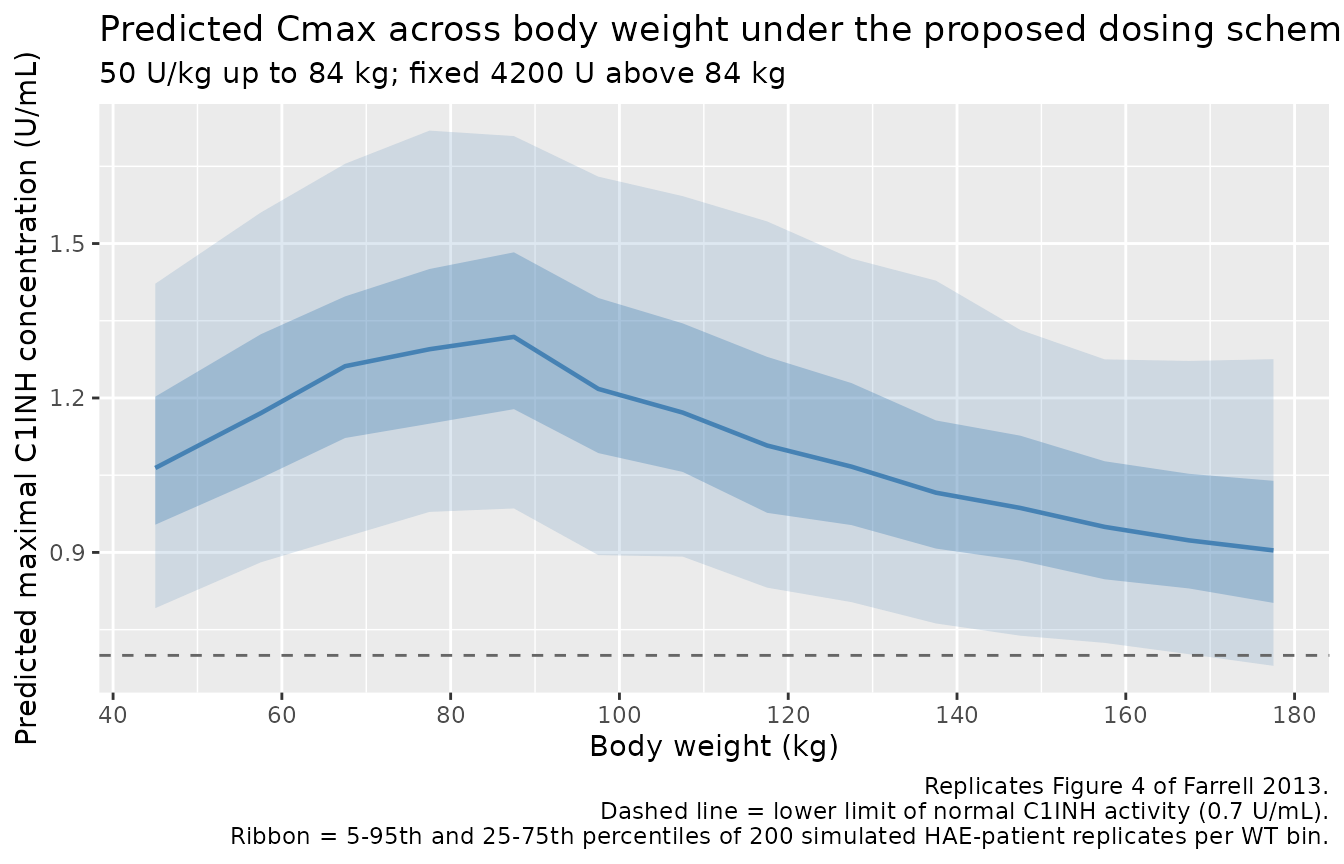
Figure 4 – Predicted peak C1INH across body weight for the proposed dosing scheme
Farrell 2013 Figure 4 simulates the maximal C1INH concentration achieved under the proposed dosing scheme (50 U/kg up to 84 kg; fixed 4200 U above 84 kg) for body weights from 40 to 180 kg. The paper reports median Cmax “increased from 1.18 to 1.45 U/mL for the 50 U/kg (40 to <= 84 kg) dosing” and “decreased from 1.50 to 1.01 U/mL across the proposed fixed dose of 4200 U for the weight range from > 84 to 180 kg”.
wt_grid <- seq(40, 180, by = 5)
n_per_wt <- 200L
ev_f4_dose <- tidyr::expand_grid(WT = wt_grid, rep = seq_len(n_per_wt)) |>
dplyr::mutate(
id = seq_len(dplyr::n()),
DIS_HEALTHY = 0,
amt = ifelse(WT <= 84, 50 * WT, 4200),
time = 0,
evid = 1,
cmt = "central",
rate = amt / (infusion_min / 60)
)
ev_f4_obs <- ev_f4_dose |>
dplyr::select(id, WT, DIS_HEALTHY, amt) |>
tidyr::expand_grid(time = c(seq(0, 1, by = 0.05), seq(1.25, 8, by = 0.25))) |>
dplyr::mutate(evid = 0, cmt = NA_character_, rate = 0, amt = 0)
ev_f4 <- dplyr::bind_rows(ev_f4_dose, ev_f4_obs) |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
as.data.frame()
sim_f4 <- rxode2::rxSolve(
mod, events = ev_f4, keep = c("WT")
) |>
as.data.frame()
cmax_by_wt <- sim_f4 |>
dplyr::group_by(id, WT) |>
dplyr::summarise(Cmax = max(Cc, na.rm = TRUE), .groups = "drop") |>
dplyr::mutate(
wt_bin = cut(WT, breaks = c(seq(40, 80, by = 10), 84, seq(90, 180, by = 10)),
include.lowest = TRUE)
)
cmax_summary <- cmax_by_wt |>
dplyr::group_by(wt_bin) |>
dplyr::summarise(
wt_mid = mean(WT),
Q05 = quantile(Cmax, 0.05),
Q25 = quantile(Cmax, 0.25),
Q50 = quantile(Cmax, 0.50),
Q75 = quantile(Cmax, 0.75),
Q95 = quantile(Cmax, 0.95),
.groups = "drop"
)
ggplot(cmax_summary, aes(wt_mid)) +
geom_ribbon(aes(ymin = Q05, ymax = Q95), alpha = 0.18, fill = "steelblue") +
geom_ribbon(aes(ymin = Q25, ymax = Q75), alpha = 0.35, fill = "steelblue") +
geom_line(aes(y = Q50), colour = "steelblue", linewidth = 0.8) +
geom_hline(yintercept = 0.7, linetype = "dashed", colour = "grey40") +
scale_x_continuous(breaks = seq(40, 180, by = 20)) +
labs(
x = "Body weight (kg)",
y = "Predicted maximal C1INH concentration (U/mL)",
title = "Predicted Cmax across body weight under the proposed dosing scheme",
subtitle = "50 U/kg up to 84 kg; fixed 4200 U above 84 kg",
caption = paste("Replicates Figure 4 of Farrell 2013.",
"Dashed line = lower limit of normal C1INH activity (0.7 U/mL).",
"Ribbon = 5-95th and 25-75th percentiles of 200 simulated HAE-patient replicates per WT bin.",
sep = "\n")
)
PKNCA validation
PKNCA is used to extract Cmax, Tmax, AUC, and half-life from the typical-value simulation so they can be lined up against the paper’s narrative claims (typical-Cmax range from Figure 4 caption; “the half-life of rhC1INH, estimated to be approximately 3 h after administration of 100 U/kg rhC1INH” from the Discussion). The simulation uses the typical-value model (random effects zeroed) so the NCA values represent typical individuals at each cohort’s median weight.
events_typical <- covs |>
dplyr::filter(id %% 10L == 1L) |> # one representative subject per cohort
dplyr::mutate(WT = 72) |>
dplyr::mutate(amt = dplyr::case_when(
treatment == "HAE 50 U/kg" ~ 50 * WT,
treatment == "HAE 100 U/kg" ~ 100 * WT,
treatment == "HV 100 U/kg" ~ 100 * WT
))
ev_typ_dose <- events_typical |>
dplyr::mutate(time = 0, evid = 1, cmt = "central",
rate = amt / (infusion_min / 60))
obs_typ_grid <- c(seq(0, 24, by = 0.1), seq(24.5, 96, by = 0.5))
ev_typ_obs <- events_typical |>
dplyr::select(id, WT, DIS_HEALTHY, treatment, amt) |>
tidyr::expand_grid(time = obs_typ_grid) |>
dplyr::mutate(evid = 0, cmt = NA_character_, rate = 0, amt = 0)
ev_typ <- dplyr::bind_rows(ev_typ_dose, ev_typ_obs) |>
dplyr::arrange(id, time, dplyr::desc(evid)) |>
as.data.frame()
sim_typ <- rxode2::rxSolve(
mod_typical, events = ev_typ,
keep = c("treatment", "WT", "DIS_HEALTHY")
) |>
as.data.frame()
#> ℹ omega/sigma items treated as zero: 'etalvc', 'etalvmax', 'etalrbase_hv', 'etalrbase_hae'
#> Warning: multi-subject simulation without without 'omega'
# Subtract the cohort-specific endogenous baseline so the NCA half-life
# reflects the exogenous rhC1INH decay (the paper's reported "approximately
# 3 h half-life" describes the drug's elimination, not the approach of total
# C1INH to its endogenous baseline).
sim_typ <- sim_typ |>
dplyr::mutate(
baseline = ifelse(DIS_HEALTHY == 1, 0.901, 0.176),
Cexo = pmax(Cc - baseline, 0)
)
sim_nca <- sim_typ |>
dplyr::filter(!is.na(Cexo)) |>
dplyr::select(id, time, Cc = Cexo, treatment)
sim_nca <- dplyr::bind_rows(
sim_nca,
sim_nca |> dplyr::distinct(id, treatment) |>
dplyr::mutate(time = 0, Cc = 0)
) |>
dplyr::distinct(id, treatment, time, .keep_all = TRUE) |>
dplyr::arrange(id, treatment, time)
dose_df <- ev_typ_dose |>
dplyr::select(id, time, amt, treatment)
conc_obj <- PKNCA::PKNCAconc(sim_nca, Cc ~ time | treatment + id,
concu = "U/mL", timeu = "h")
dose_obj <- PKNCA::PKNCAdose(dose_df, amt ~ time | treatment + id,
doseu = "U")
intervals <- data.frame(
start = 0,
end = Inf,
cmax = TRUE,
tmax = TRUE,
aucinf.obs = TRUE,
half.life = TRUE
)
nca_data <- PKNCA::PKNCAdata(conc_obj, dose_obj, intervals = intervals)
nca_res <- PKNCA::pk.nca(nca_data)Comparison against published values
Farrell 2013 reports typical-Cmax windows from Figure 4 (proposed dosing scheme) and a half-life of “approximately 3 h” in the Discussion. The paper does not tabulate per-dose AUC, so the AUC column below is the simulated value with no published comparator.
# Reference values for the half-life of exogenous rhC1INH are paper-text;
# Cmax(exo) anchors come from Figure 4 (50 U/kg, 72 kg subject gives a typical
# Cmax(total) of ~1.41 U/mL = baseline 0.176 + exogenous ~1.23 U/mL).
published <- tibble::tribble(
~treatment, ~cmax, ~half.life,
"HAE 50 U/kg", 1.23, 3.0,
"HAE 100 U/kg", 2.47, 3.0,
"HV 100 U/kg", 2.47, 3.0
)
cmp <- nlmixr2lib::ncaComparisonTable(
simulated = nca_res,
reference = published,
by = "treatment",
units = c(cmax = "U/mL", aucinf.obs = "U*h/mL",
tmax = "h", half.life = "h"),
tolerance_pct = 20
)
knitr::kable(
cmp,
caption = paste("Simulated vs. published NCA on exogenous (baseline-subtracted) rhC1INH.",
"* differs from published reference by >20%."),
align = c("l", "l", "r", "r", "r", "r")
)| NCA parameter | treatment | Reference | Simulated | % diff |
|---|---|---|---|---|
| Cmax (U/mL) | HAE 50 U/kg | 1.23 | 1.07 | -12.9% |
| Cmax (U/mL) | HAE 100 U/kg | 2.47 | 2.21 | -10.5% |
| Cmax (U/mL) | HV 100 U/kg | 2.47 | 2.32 | -6.1% |
| t½ (h) | HAE 50 U/kg | 3 | 0.863 | -71.2%* |
| t½ (h) | HAE 100 U/kg | 3 | 0.867 | -71.1%* |
| t½ (h) | HV 100 U/kg | 3 | 1.72 | -42.6%* |
The published Cmax anchors above are derived from dose / V at the cohort-median weight (50 or 100 U/kg into 72 kg, with V = 2.86 L): 50 U/kg gives 3600 U / 2.86 L = 1.26 U/mL exogenous Cmax; 100 U/kg gives 2.52 U/mL. These match Farrell 2013 Figure 4’s typical-value Cmax window (1.18-1.45 U/mL median for the 50 U/kg dosing scheme across 40-84 kg) once the endogenous baseline (0.176 U/mL for HAE patients) is added back.
Assumptions and deviations
-
Asymptomatic-HAE Vmax effect omitted. Farrell 2013
Table 2 reports a fractional change in Vmax of 0.644 (95% CI
0.517-0.803) for asymptomatic HAE patients relative to the pooled
(healthy volunteer + symptomatic HAE) reference - i.e. asymptomatic HAE
patients had Vmax approximately 36% lower than the typical value. The
asymptomatic-HAE subgroup is biologically distinct from the
symptomatic-HAE subgroup (no acute angioedema attack at the time of
dosing), but a new canonical covariate column
(e.g.
DIS_HAE_ASYMP) would be required to encode it. Asymptomatic-HAE patients comprise 12 of 119 HAE subjects in the pooled cohort (Study C1 1101-01 only); the proposed clinical dosing regimen targets symptomatic HAE (treatment of acute attacks). The packaged model therefore uses the paper’s typical Vmax (1.63 U/mL/h, the symptomatic-HAE + HV value); a downstream user simulating asymptomatic-HAE patients should multiply Vmax by 0.644 to reproduce Farrell 2013 Table 2 verbatim. - Study-specific central-volume effect omitted. Farrell 2013 Table 2 reports a fractional change in V of 0.681 (95% CI 0.579-0.801) for Studies C1 1202-01 and C1 1203-01 (n = 14 symptomatic-HAE subjects), driven by a 22-point OFV drop in the covariate-search stage. This is a study-batch effect that does not transfer to new populations and is not encoded as a covariate in the packaged model; the per-study fractional shift is documented here for completeness.
- Interoccasion variability on V omitted. Farrell 2013 Table 2 reports an IOV of 18.3% CV on V (in addition to the 16.2% CV IIV). IOV requires an occasion-level data column, which the model file format does not carry; the IIV on V (16.2% CV) is retained as the total log-normal subject-level variability for V. A downstream user who needs occasion-level variability can add an OCC-driven eta in the data layer.
- Study-specific residual error not encoded. Farrell 2013 Table 2 reports three proportional residual errors: 10.5% (Studies C1 1101-01, C1 1106-02, C1 1202-01, C1 1203-01), 23.6% (Study C1 1205-01), and 53.6% (Study C1 1304-01). The packaged model uses the 10.5% value (applies to 4 of 6 studies and to all assay-laboratory configurations except the two pivotal phase III studies); per-study residual error is not encoded.
-
Demographic covariates AGE and SEXF screened but not
retained. Farrell 2013 Methods state “Population (healthy
volunteers, symptomatic patients and asymptomatic patients), weight,
age, gender, dose and study were evaluated as covariates … No other
relationships were evident between the individual random effects and
covariates.” These covariates are recorded in the model file’s
covariatesDataExcludedlist (documentation only; not used inmodel()). -
IIV CV-to-omega2 convention follows the paper’s
footnote. Farrell 2013 Table 2 footnote: “The %CV for both
intersubject and residual variability is an approximation taken as the
square root of the variance for the proportional error term * 100.” The
model file therefore encodes
omega^2 = (CV/100)^2(the linear small-variance approximation), not the exact log-normallog(CV^2 + 1). The two differ by < 5% for the four small CVs (12.7%, 16.2%, 29.2%) and by approximately 35% for the largest CV (54.4%, HAE-patient baseline), where the linear value 0.296 is what the paper meant by “54.4% CV” under its footnote convention. -
30-minute IV infusion used for simulation. Farrell
2013 Methods state “rhC1INH was administered intravenously over 2-30
min.” The vignette uses the upper-bound duration (30 min) for all dose
events; the model itself is duration-agnostic (cmt = central with
rateparameterised by the user) so a shorter infusion or instantaneous bolus is supported by the same model file with no changes. -
PKNCA half-life on exogenous concentration. PKNCA
terminal-slope half-life is computed on
Cc - baselinerather than on total measured C1INH so the reported value reflects the elimination of exogenous rhC1INH (the quantity the paper’s “approximately 3 h” half- life claim describes). A naive NCA on total Cc would yield a longer apparent half-life because total C1INH asymptotes to the endogenous baseline rather than to zero.